Are you a resident of Nevada looking to know more about Form FA 27? Look no further! This blog post is dedicated to providing comprehensive and up-to-date information about the Nevada form, including who must fill it out, when to file it, where to send it and other important matters related to this document. Our goal is for you walk away from this article with a greater understanding of all that's involved with the form so that you can complete the process quickly and accurately. So let's dive in – we have everything laid out for you here so read on for more information about Form FA 27!
| Question | Answer |
|---|---|
| Form Name | Nevada Form Fa 27 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | HP, NPI, ICD-9, Revocation |
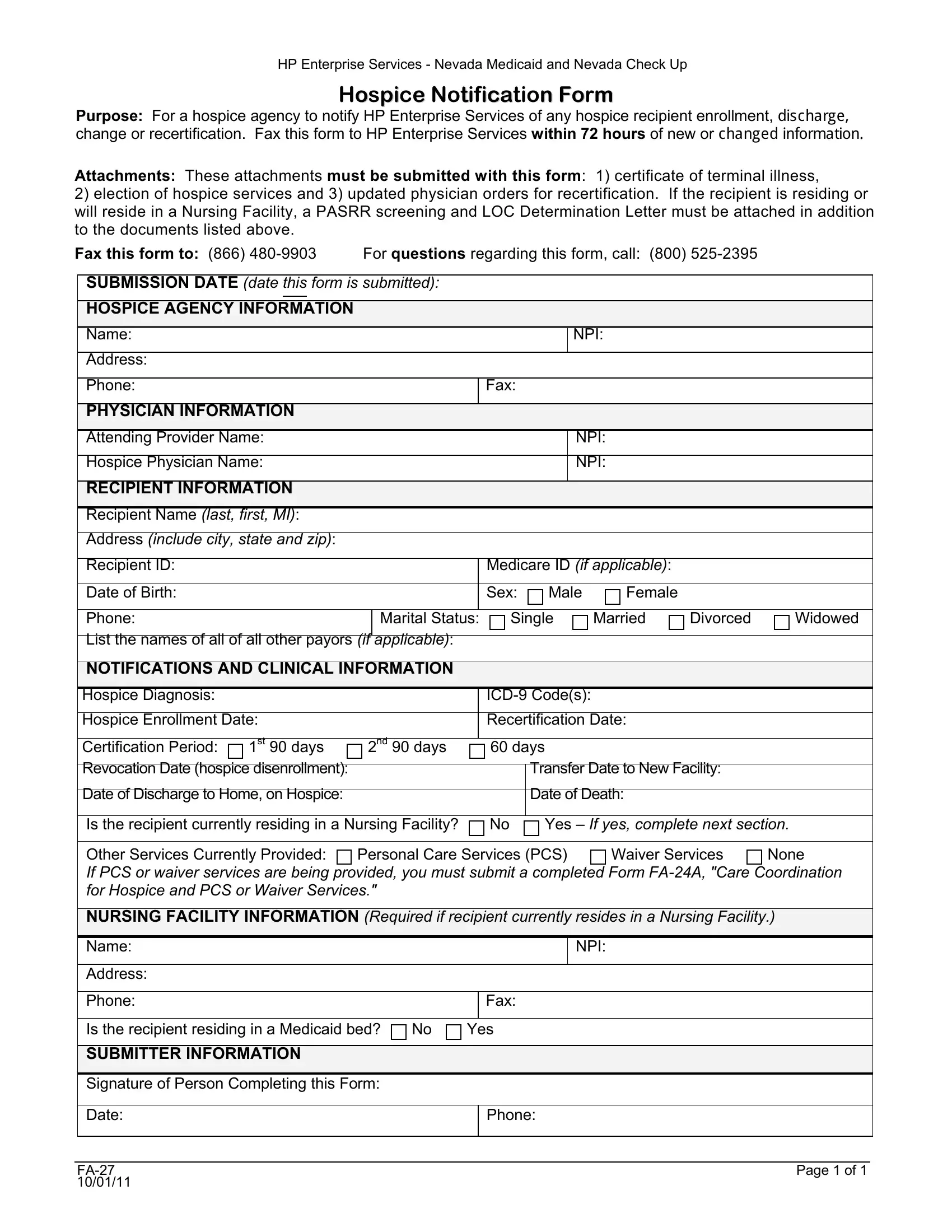
HP Enterprise Services - Nevada Medicaid and Nevada Check Up
Hospice Notification Form
Purpose: For a hospice agency to notify HP Enterprise Services of any hospice recipient enrollment, GLVFKDUJH change or recertification. Fax this form to HP Enterprise Services within 72 hours of new or FKDQJHG LQIRUPDWLRQ
Attachments: These attachments must be submitted with this form: 1) certificate of terminal illness,
2)election of hospice services and 3) updated physician orders for recertification. If the recipient is residing or will reside in a Nursing Facility, a PASRR screening and LOC Determination Letter must be attached in addition to the documents listed above.
Fax this form to: (866) |
For questions regarding this form, call: |
(800) |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
SUBMISSION DATE (date this form is submitted): |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
HOSPICE AGENCY INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
NPI: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
|
|
|
|
|
|
Fax: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
PHYSICIAN INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Attending Provider Name: |
|
|
|
|
|
|
|
|
NPI: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Hospice Physician Name: |
|
|
|
|
|
|
|
|
NPI: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
RECIPIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recipient Name (last, first, MI): |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Address (include city, state and zip): |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Recipient ID: |
|
|
|
|
|
|
|
|
|
Medicare ID (if applicable): |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Date of Birth: |
|
|
|
|
|
|
|
|
|
Sex: |
Male |
Female |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Phone: |
|
|
|
|
|
Marital Status: |
|
Single |
Married |
Divorced |
Widowed |
||||
|
List the names of all of all other payors (if |
|
applicable): |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
NOTIFICATIONS AND CLINICAL INFORMATION |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hospice Diagnosis: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Hospice Enrollment Date: |
|
|
|
|
|
|
Recertification Date: |
|
|
||||||
|
Certification Period: |
1st 90 days |
2nd 90 days |
|
|
60 days |
|
|
|
|||||||
|
|
|
|
|
|
|||||||||||
|
Revocation Date (hospice disenrollment): |
|
|
|
|
|
|
|
Transfer Date to New Facility: |
|
||||||
|
|
|
|
|
|
|
|
|
||||||||
|
Date of Discharge to Home, on Hospice: |
|
|
|
|
|
|
|
Date of Death: |
|
|
|||||
|
|
|
|
|
|
|||||||||||
|
Is the recipient currently residing in a Nursing Facility? |
|
|
No |
Yes – If yes, complete next section. |
|||||||||||
|
|
|
|
|
||||||||||||
|
Other Services Currently Provided: |
Personal Care Services (PCS) |
Waiver Services |
None |
||||||||||||
|
If PCS or waiver services are being provided, you must submit a completed Form |
|||||||||||||||
|
for Hospice and PCS or Waiver Services." |
|
|
|
|
|
|
|
|
|
||||||
|
|
|||||||||||||||
|
NURSING FACILITY INFORMATION (Required if recipient currently resides in a Nursing Facility.) |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
NPI: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
|
|
|
|
|
|
Fax: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Is the recipient residing in a Medicaid bed? |
No |
Yes |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
SUBMITTER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Person Completing this Form: |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Date: |
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 1 of 1 |
|
0/01/11 |
|