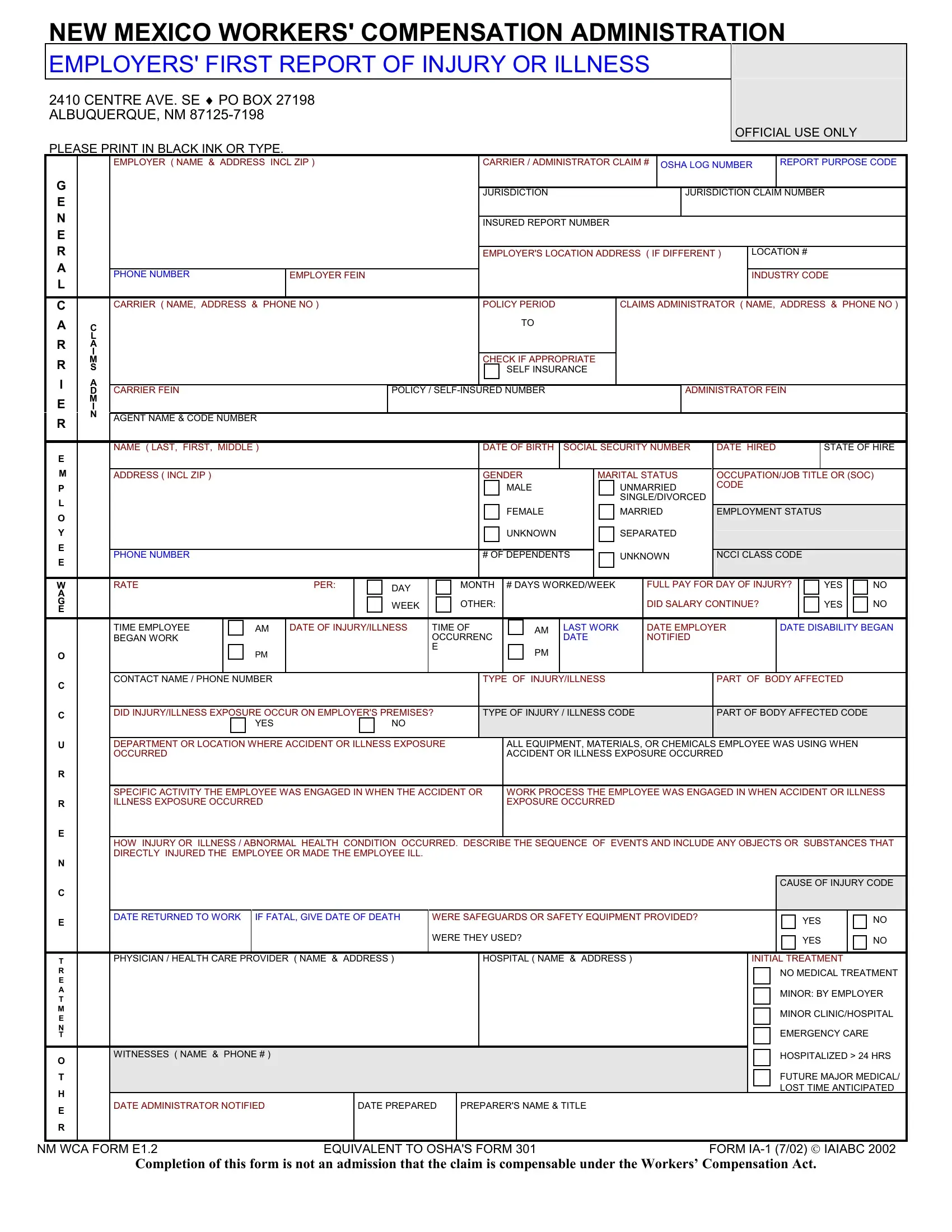
The New Mexico Workers' Compensation Administration mandates the use of the Employers' First Report of Injury or Illness form to ensure meticulous documentation and timely reporting of workplace accidents or illnesses. Situated at 2410 Centre Ave. SE, Albuquerque, with additional offices statewide, this form serves as a vital tool in managing workers' compensation claims, underlining the importance of accuracy and detail in reporting. Employers must complete this form in black ink or type, providing comprehensive details about the employee involved, the nature of the injury or illness, and circumstances under which it occurred. The form covers a wide range of information, including employer and carrier details, the injured or ill employee’s personal and employment information, specifics about the injury or illness, treatment received, and witnesses, if any. It also prompts for the inclusion of codes relevant to the industry and injury type, underpinning the structured assessment and processing of the claim. This documentation is crucial not only for immediate medical response and compensation but also for improving workplace safety and prevention strategies. Employers are encouraged to fill in even the optional shaded areas for a fuller record that could be beneficial for internal use. Filing within the stiperset timelines and ensuring the provision of copies to all relevant parties, including the worker and the compensation insurer, is emphasized to avoid penalties. This form acts as neither an admission of liability nor a denial of the claim's compensability but as a foundational step in the workers' compensation process, ensuring all parties are adequately informed and rights are observed.
| Question | Answer |
|---|---|
| Form Name | New Mexico Form Report |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | new mexico hire report form, form mexico new report, new mexico first report of injury form, nm form compensation |