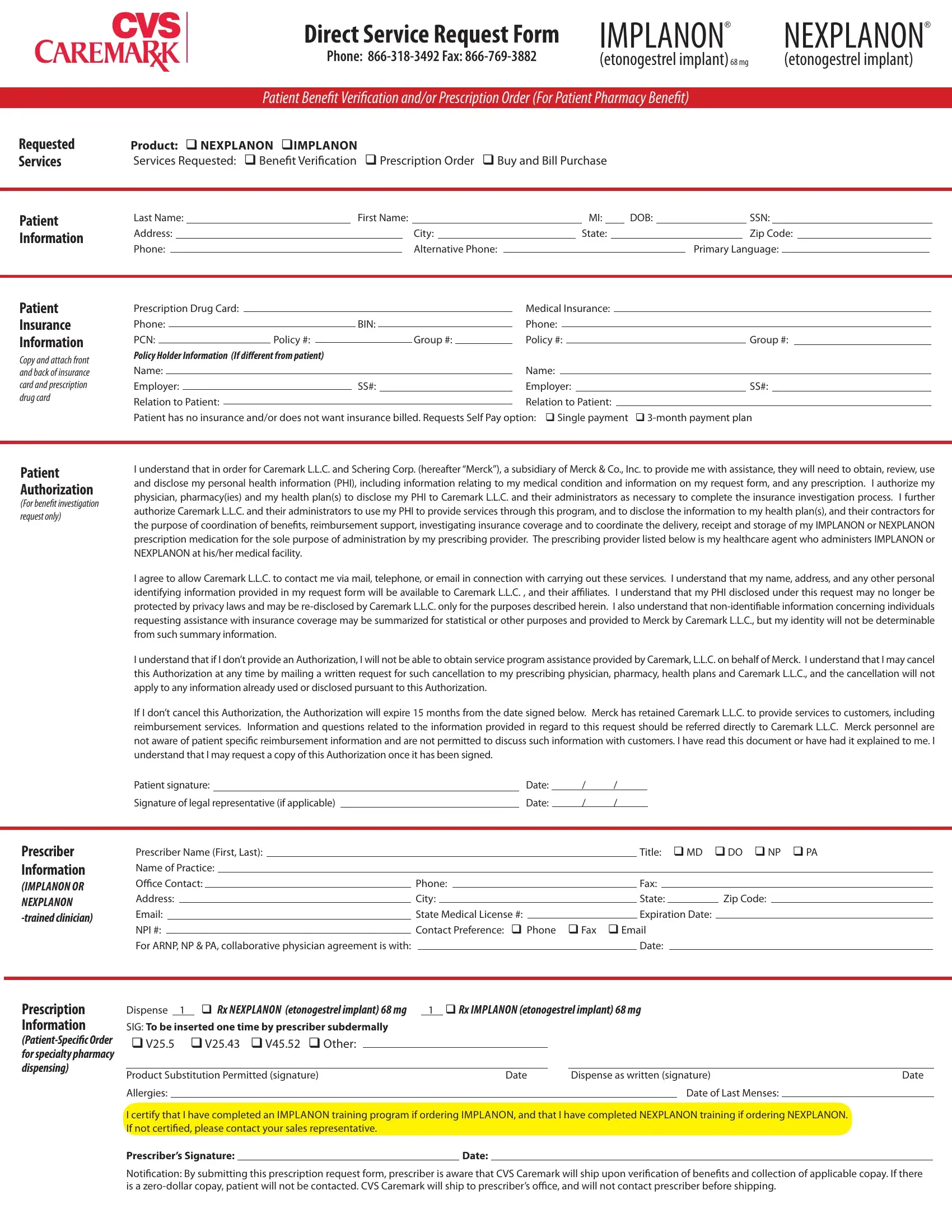
When it comes to managing reproductive health and family planning options, individuals often seek the most convenient and effective solutions. The Nexplanon CVS form serves a pivotal role in streamlining access to one such solution, providing a direct service request form for IMPLANON® and NEXPLANON® (etonogestrel implant)68 mg. This comprehensive form caters to patient benefit verification, prescription orders, and buy and bill purchases, ensuring that both patients and prescribers have a seamless process for obtaining these implants. With fields for patient information, insurance details, and prescriber credentials, the form facilitates a thorough scrutiny of benefits and covers all bases from prescription requests to delivery arrangements. Moreover, it underscores the importance of patient consent and authorization for using personal health information, a crucial step for privacy and transparency. The integration of insurance investigation, benefit coordination, and prescription medication delivery into one form reflects a tailored approach to healthcare provision, aiming to expedite and simplify the process for everyone involved.
| Question | Answer |
|---|---|
| Form Name | Nexplanon Cvs Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | merck nexplanon enrollment form 2021, nexplanon form, nexplanon application form 2021, nexplanon form 2021 |