Having the objective of making it as easy to go with as it can be, we established our PDF editor. The procedure of completing the nih 527 sp is going to be very simple in the event you check out the next actions.
Step 1: Search for the button "Get Form Here" on the site and hit it.
Step 2: Once you enter the nih 527 sp editing page, you'll see each of the functions you can take about your document within the top menu.
These parts will frame the PDF document that you'll be creating:
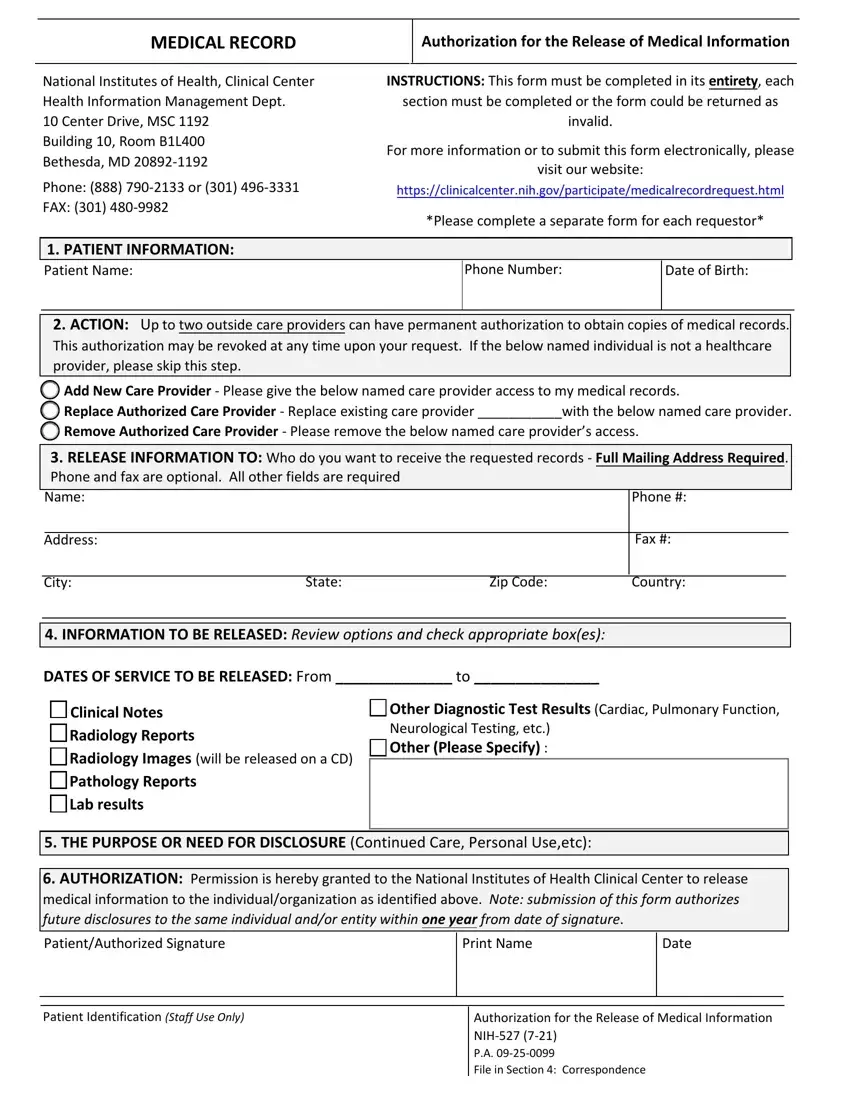
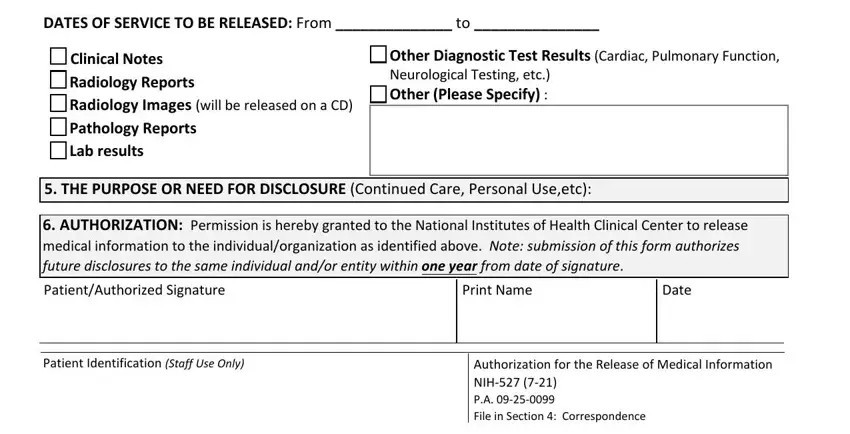
The application will need you to fill in the DATES OF SERVICE TO BE RELEASED, Clinical Notes Radiology Reports, Other Diagnostic Test Results, Neurological Testing etc Other, THE PURPOSE OR NEED FOR, AUTHORIZATION Permission is, PatientAuthorized Signature, Print Name, Date, Patient Identification Staff Use, and Authorization for the Release of segment.
Step 3: Press the Done button to save your document. So now it is readily available for upload to your device.
Step 4: Make copies of your document - it can help you stay away from forthcoming troubles. And don't be concerned - we do not distribute or see your data.
