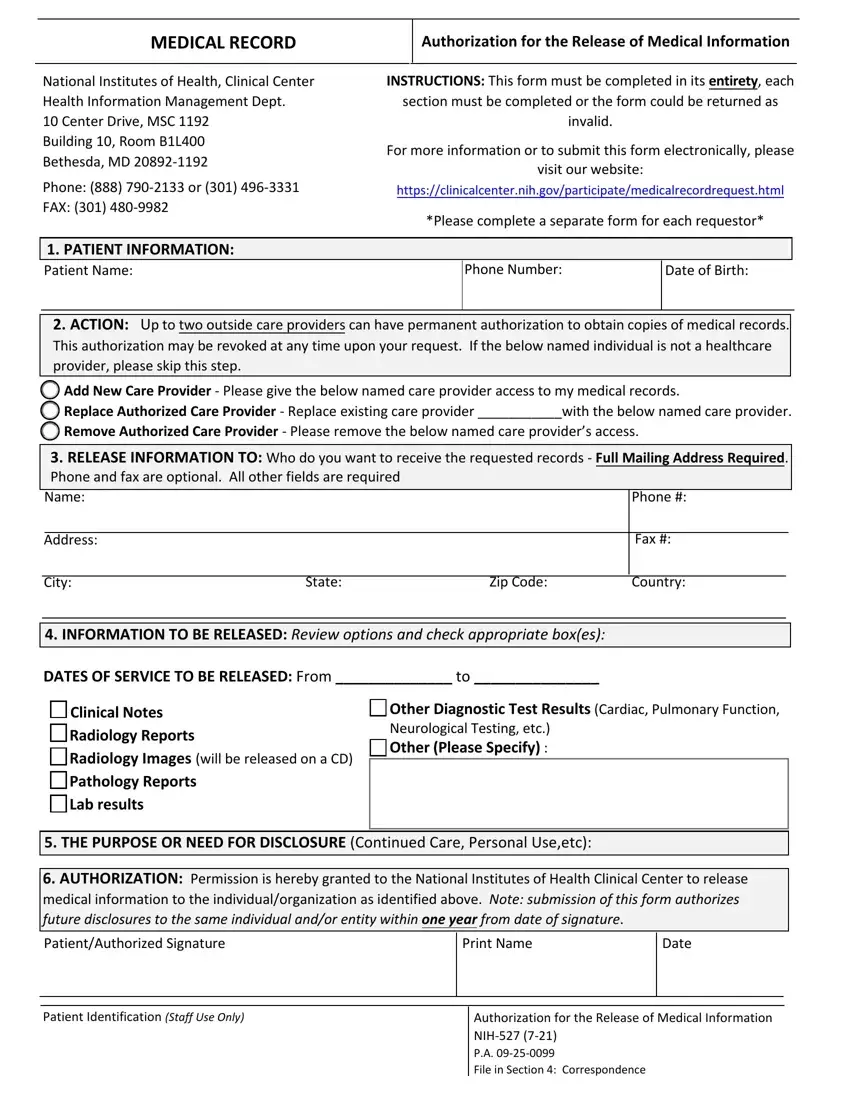
When navigating the complexities of obtaining medical records or authorizing their release to healthcare providers, the National Institutes of Health (NIH) 527 form plays a crucial role. This form is an essential tool used within the NIH Clinical Center for patients who wish to have their medical records released or to grant permission for their healthcare providers to access these records. Specifically designed to ensure patient privacy while facilitating the seamless sharing of vital medical information, the NIH 527 form requires comprehensive details to be filled out. This includes patient information, actions permitting or altering access to records by healthcare providers, and specifics about the type or extent of medical information to be released. Additionally, it outlines how to submit the form electronically, enhancing its accessibility for patients and their families. Notably, the form allows patients to authorize up to two outside care providers to obtain copies of their medical records permanently, which can be revoked at any time based on the patient's discretion. However, the form underscores the importance of completing every section thoroughly to avoid it being returned as invalid. It also highlights the need for specifying the purpose of the disclosure, whether for continued care, personal use, or another reason, ensuring that the release of information is tightly controlled and explicitly consented to by the patient.
| Question | Answer |
|---|---|
| Form Name | Nih 527 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | nih medical records, nih patient information, nih records, nih527 |
