
 YYYY
YYYY
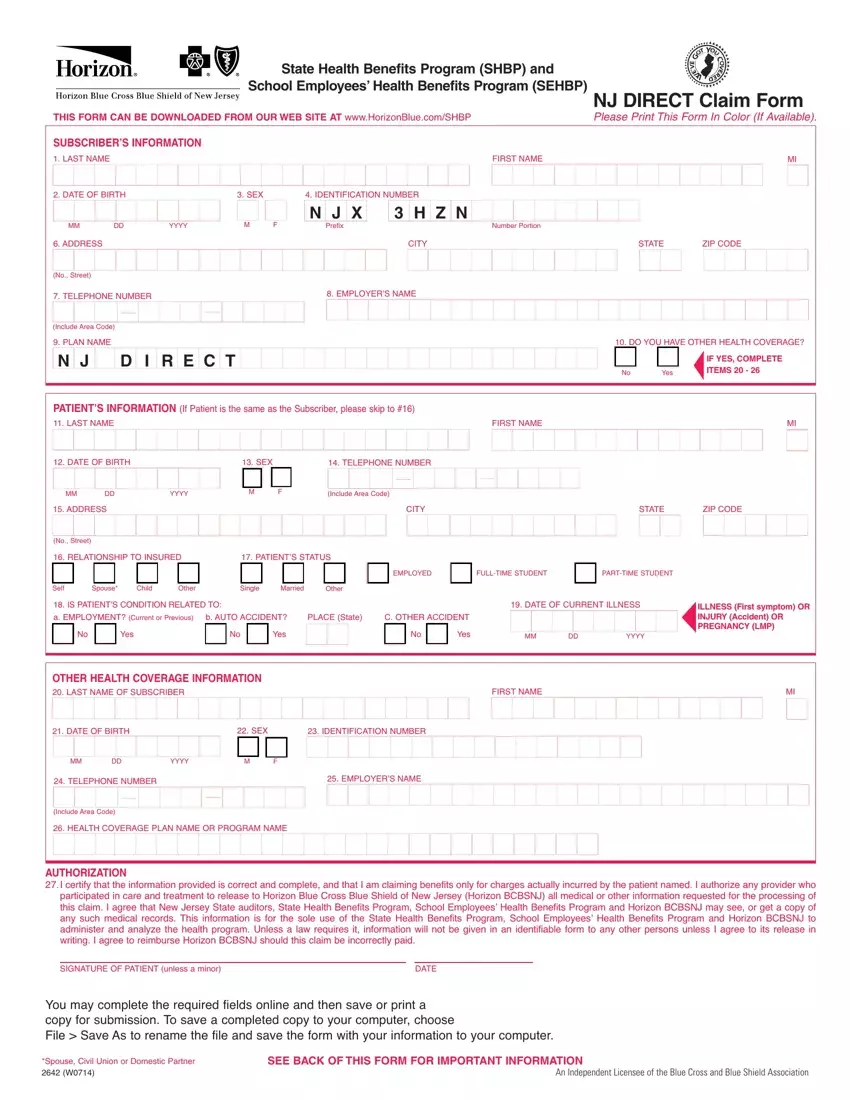
You can easily fill in forms applying our PDF editor. Modifying the claim form nj file is not difficult should you consider these steps:
Step 1: You should choose the orange "Get Form Now" button at the top of the following webpage.
Step 2: Now you should be on the document edit page. You can add, customize, highlight, check, cross, add or remove areas or phrases.
Feel free to enter the following details to complete the claim form nj PDF:
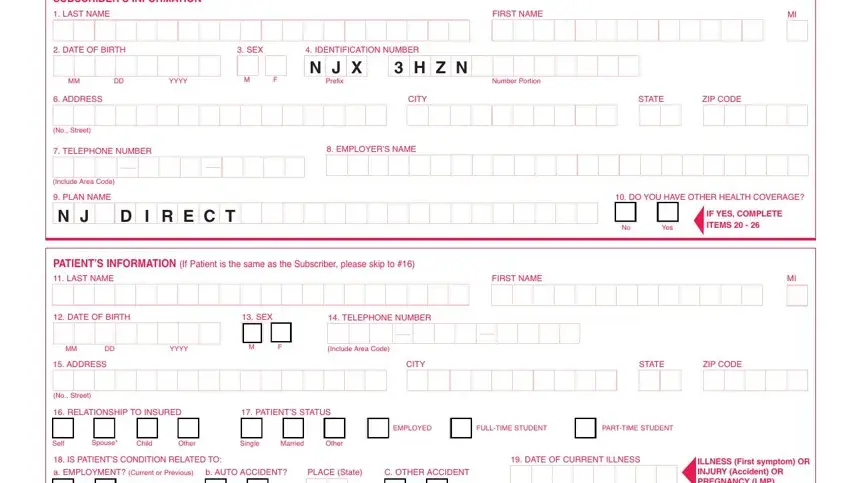
Remember to provide the information inside the segment OTHER HEALTH COVERAGE INFORMATION, LAST NAME OF SUBSCRIBER, FIRST NAME, DATE OF BIRTH, SEX, IDENTIFICATION NUMBER, YYYY, TELEPHONE NUMBER, EMPLOYERS NAME, Include Area Code, HEALTH COVERAGE PLAN NAME OR, AUTHORIZATION, I certify that the information, SIGNATURE OF PATIENT unless a, and DATE.
Step 3: Click the button "Done". Your PDF document can be exported. You can save it to your pc or send it by email.
Step 4: Get duplicates of the document. This may protect you from potential worries. We don't look at or distribute your information, for that reason you can relax knowing it's going to be secure.
