

Dealing with PDF files online is definitely simple with this PDF tool. Anyone can fill in Northwestern Life Insurance Change Of Beneficiary Form here painlessly. The editor is continually updated by our team, getting handy functions and becoming greater. For anyone who is looking to get started, here's what it will require:
Step 1: Click on the "Get Form" button above on this page to open our editor.
Step 2: As you open the editor, you will notice the document all set to be filled out. In addition to filling out different blank fields, it's also possible to do other sorts of actions with the PDF, specifically adding any textual content, changing the initial text, inserting illustrations or photos, signing the PDF, and a lot more.
It's straightforward to complete the document using out detailed tutorial! This is what you must do:
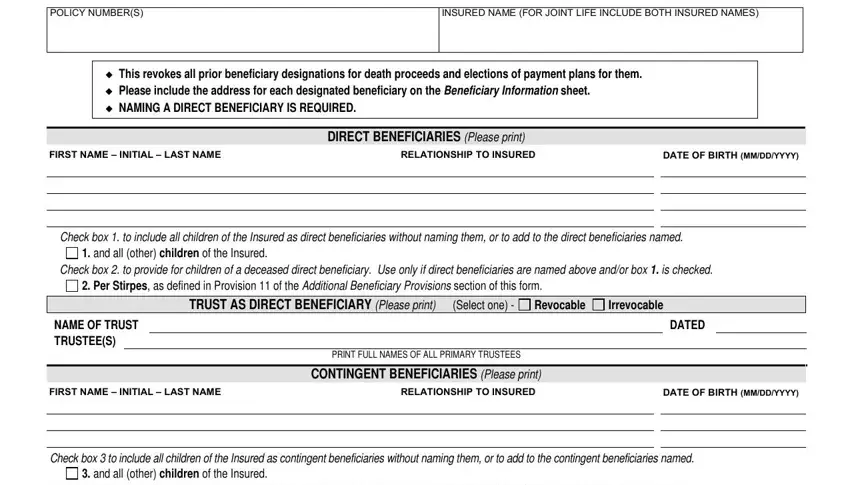
1. You should fill out the Northwestern Life Insurance Change Of Beneficiary Form correctly, so be mindful while working with the parts that contain all these fields:
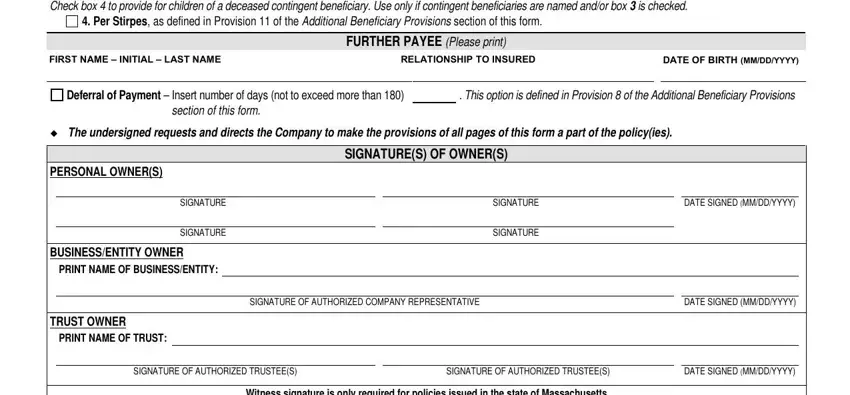
2. When this section is completed, you'll want to insert the essential specifics in Check box to provide for children, Per Stirpes as defined in, FIRST NAME INITIAL LAST NAME, FURTHER PAYEE Please print, RELATIONSHIP TO INSURED, DATE OF BIRTH MMDDYYYY, Deferral of Payment Insert number, This option is defined in, section of this form, The undersigned requests and, PERSONAL OWNERS, SIGNATURE, SIGNATURE, BUSINESSENTITY OWNER PRINT NAME OF, and SIGNATURES OF OWNERS so that you can proceed further.
3. Your next step is simple - fill out all the empty fields in WITNESS SIGNATURE, Witness signature is only required, WITNESS SIGNATURE MAY NOT BE A, PRINT NAME, and Page of FEfl to complete this part.

4. You're ready to begin working on this fourth section! Here you will have all these TRUSTEE AS BENEFICIARY If a, AMENDMENT OF POLICY PROVISIONS, A Policies Numbered below, The policy is amended to delete, payment plan, provide that a payment plan for, the Insured is living in all other, provide that the Company is not, Provisions in the policy regarding, provide that the Company may, B Policies Numbered below, and Page of FEfl blanks to fill out.
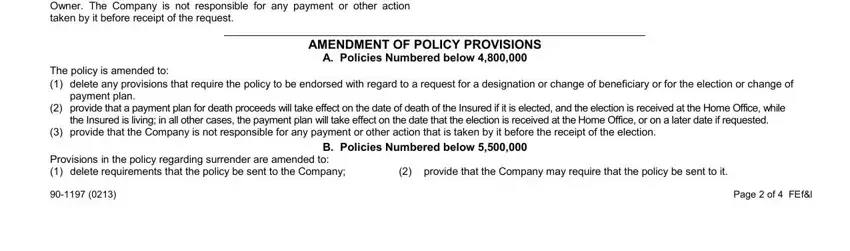
People generally make mistakes while filling out the Insured is living in all other in this section. Be sure you reread what you enter here.
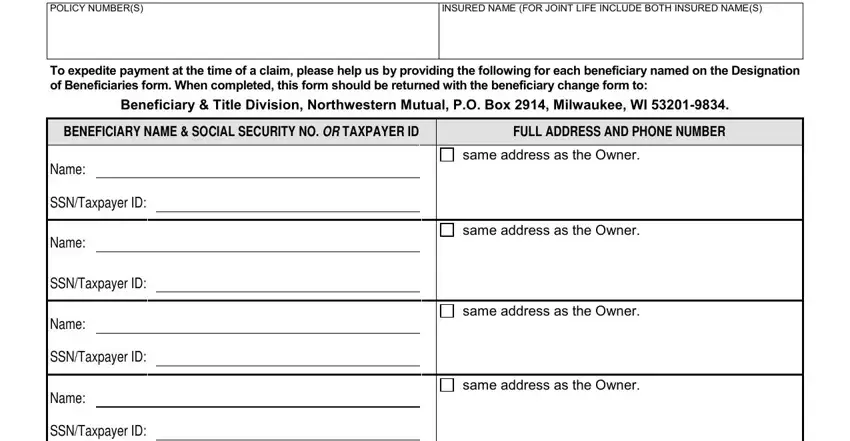
5. This final section to complete this PDF form is critical. Be sure to fill in the displayed form fields, such as POLICY NUMBERS, INSURED NAME FOR JOINT LIFE, To expedite payment at the time of, Beneficiary Title Division, BENEFICIARY NAME SOCIAL SECURITY, FULL ADDRESS AND PHONE NUMBER, Name, SSNTaxpayer ID, Name, SSNTaxpayer ID, Name, SSNTaxpayer ID, Name, SSNTaxpayer ID, and same address as the Owner, prior to finalizing. Failing to do this might generate an incomplete and possibly unacceptable form!
Step 3: Before finishing your file, double-check that all blanks are filled out right. The moment you establish that it's correct, press “Done." Join FormsPal today and immediately get Northwestern Life Insurance Change Of Beneficiary Form, all set for downloading. Each edit you make is handily preserved , helping you to edit the form later if required. When using FormsPal, you're able to fill out documents without having to get worried about database leaks or data entries being distributed. Our secure system helps to ensure that your personal data is maintained safe.