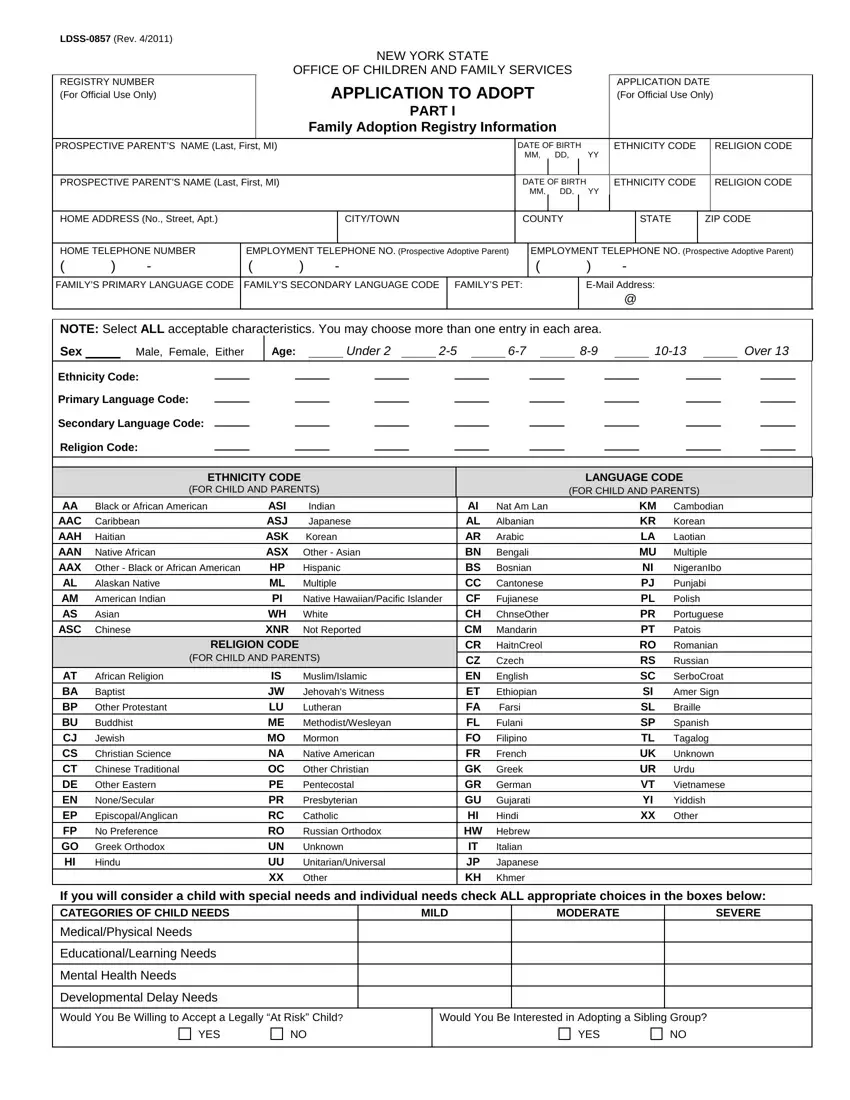
The New York State Adoption Form, officially known as LDSS-0857 (Rev. 4/2011), serves as an essential touchpoint for prospective adoptive parents navigating the adoption process. Crafted by the New York State Office of Children and Family Services, this comprehensive document embarks on gathering intricate details about prospective parents, aiming to facilitate a successful match between them and a child awaiting adoption. It categorizes essential personal information, including names, dates of birth, employment details, language preferences, and more, thus painting a detailed picture of the prospective adoptive family’s background. Additionally, the form thoughtfully inquires about the prospective parents' openness to embracing a child with specific characteristics such as age, gender, ethnicity, and special needs, indicating a commitment to accommodating the diverse needs and preferences of children in foster care. The adoption process’s complexity is further unpacked through sections that delve into the family’s home environment, their willingness to adopt siblings or children considered “at risk,” and the status of their homestudy process. Critical legal notes embedded within the form remind applicants of their rights and obligations, underline the importance of a thorough background check, and explain the procedure for seeking redress through a State administrative hearing should there be complications or concerns. This form not only serves as a gateway to the transformative journey of adoption but also underscores the state’s dedication to ensuring that the children’s best interests are at the forefront of all adoption proceedings.
| Question | Answer |
|---|---|
| Form Name | Ny Adoption Form |
| Form Length | 7 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 45 sec |
| Other names | ny 27 a form, 27a petition form, ny adoption form online, ny adoption a form |
|
|
|
|
|
|
|
NEW YORK STATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OFFICE OF CHILDREN AND FAMILY SERVICES |
|
|
|
|
|
|||||||
REGISTRY NUMBER |
|
|
|
APPLICATION TO ADOPT |
|
APPLICATION DATE |
|||||||||||
(For Official Use Only) |
|
|
|
|
(For Official Use Only) |
||||||||||||
|
|
|
|
|
|
|
PART I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Family Adoption Registry Information |
|
|
|
|
|
||||||
PROSPECTIVE PARENT’S NAME (Last, First, MI) |
|
|
|
|
DATE OF BIRTH |
YY |
ETHNICITY CODE |
|
RELIGION CODE |
||||||||
|
|
|
|
|
|
|
|
|
MM, DD, |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
PROSPECTIVE PARENT’S NAME (Last, First, MI) |
|
|
|
|
DATE OF BIRTH |
ETHNICITY CODE |
|
RELIGION CODE |
|||||||||
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
MM, DD, YY |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
HOME ADDRESS (No., Street, Apt.) |
|
|
|
|
CITY/TOWN |
COUNTY |
|
|
STATE |
ZIP CODE |
|||||||
|
|
|
|
|
|
|
|
||||||||||
HOME TELEPHONE NUMBER |
EMPLOYMENT TELEPHONE NO. (Prospective Adoptive Parent) |
|
EMPLOYMENT TELEPHONE NO. (Prospective Adoptive Parent) |
||||||||||||||
( |
) |
- |
( |
|
) |
- |
|
|
( |
|
|
) |
- |
|
|
|
|
FAMILY’S PRIMARY LANGUAGE CODE |
FAMILY’S SECONDARY LANGUAGE CODE |
FAMILY’S PET: |
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
@ |
|
|
|
NOTE: Select ALL acceptable characteristics. You may choose more than one entry in each area.
Sex Male, Female, Either
Age: |
|
Under 2 |
|
|
|
|
|
Over 13 |
Ethnicity Code:
Primary Language Code:
Secondary Language Code:
Religion Code:
ETHNICITY CODE
(FOR CHILD AND PARENTS)
LANGUAGE CODE
(FOR CHILD AND PARENTS)
AA |
Black or African American |
ASI |
Indian |
AI |
Nat Am Lan |
KM |
Cambodian |
|
AAC |
Caribbean |
ASJ |
Japanese |
AL |
Albanian |
KR |
Korean |
|
AAH |
Haitian |
ASK |
Korean |
AR |
Arabic |
LA |
Laotian |
|
AAN |
Native African |
ASX |
Other - Asian |
BN |
Bengali |
MU |
Multiple |
|
AAX |
Other - Black or African American |
HP |
Hispanic |
BS |
Bosnian |
NI |
NigeranIbo |
|
AL |
Alaskan Native |
ML |
Multiple |
CC |
Cantonese |
PJ |
Punjabi |
|
AM |
American Indian |
PI |
Native Hawaiian/Pacific Islander |
CF |
Fujianese |
PL |
Polish |
|
AS |
Asian |
WH |
White |
CH |
ChnseOther |
PR |
Portuguese |
|
ASC |
Chinese |
XNR |
Not Reported |
CM |
Mandarin |
PT |
Patois |
|
|
RELIGION CODE |
|
|
CR |
HaitnCreol |
RO |
Romanian |
|
|
(FOR CHILD AND PARENTS) |
|
CZ |
Czech |
RS |
Russian |
||
AT |
African Religion |
IS |
Muslim/Islamic |
EN |
English |
SC |
SerboCroat |
|
BA |
Baptist |
JW |
Jehovah's Witness |
ET |
Ethiopian |
SI |
Amer Sign |
|
BP |
Other Protestant |
LU |
Lutheran |
FA |
Farsi |
SL |
Braille |
|
BU |
Buddhist |
ME |
Methodist/Wesleyan |
FL |
Fulani |
SP |
Spanish |
|
CJ |
Jewish |
MO |
Mormon |
FO |
Filipino |
TL |
Tagalog |
|
CS |
Christian Science |
NA |
Native American |
FR |
French |
UK |
Unknown |
|
CT |
Chinese Traditional |
OC |
Other Christian |
GK |
Greek |
UR |
Urdu |
|
DE |
Other Eastern |
PE |
Pentecostal |
GR |
German |
VT |
Vietnamese |
|
EN |
None/Secular |
PR |
Presbyterian |
GU |
Gujarati |
YI |
Yiddish |
|
EP |
Episcopal/Anglican |
RC |
Catholic |
HI |
Hindi |
XX |
Other |
|
FP |
No Preference |
RO |
Russian Orthodox |
HW |
Hebrew |
|
|
|
GO |
Greek Orthodox |
UN |
Unknown |
IT |
Italian |
|
|
|
HI |
Hindu |
UU |
Unitarian/Universal |
JP |
Japanese |
|
|
|
|
|
XX |
Other |
KH |
Khmer |
|
|
|
If you will consider a child with special needs and individual needs check ALL appropriate choices in the boxes below:
CATEGORIES OF CHILD NEEDS
Medical/Physical Needs
Educational/Learning Needs
Mental Health Needs
Developmental Delay Needs
MILD
MODERATE
SEVERE
Would You Be Willing to Accept a Legally “At Risk” Child?
YESNO
Would You Be Interested in Adopting a Sibling Group?
YESNO
NEW YORK STATE
OFFICE OF CHILDREN AND FAMILY SERVICES
FAMILY CERTIFICATION INFORMATION
PART II
Are you currently an approved adoptive parent?
Yes |
No |
If yes, please provide approval date:
MM
DD
YY
NAME OF AGENCY
CONTACT PERSON
TELEPHONE NUMBER
( ) -
AGENCY ADDRESS (NO., STREET, APT.)
CITY/TOWN
COUNTY
STATE
ZIP CODE
IF YOU DO NOT HAVE A COMPLETED HOMESTUDY AND WOULD LIKE TO BEGIN THE HOMESTUDY PROCESS, PLEASE GIVE COMPLETE INSTRUCTIONS FOR REACHING YOUR HOME:
FOR OFFICIAL USE ONLY
HOME STUDY STATUS |
|
|
|
1. In Process |
2. Completed Favorable |
3. Completed Unfavorable |
4. Discontinued |
GENERAL FAMILY INFORMATION
PART III
(To be completed by applicant)
IS THERE A FOSTER CHILD FREED FOR |
DO YOU WISH TO ADOPT WHAT IS THE CHILD’S FULL NAME? |
ADOPTION CURRENTLY LIVING IN YOUR HOME? |
THIS CHILD? |
Yes |
No |
|
Yes |
|
No |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
CHILD’S DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
DATE OF PLACEMENT |
|
|
|
|
|
|
|
|
MM |
DD |
YY |
|
|
MM |
|
DD |
|
YY |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
CURRENT MARRIAGE INFORMATION |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
CURRENT MARRIAGE PLACE |
|
|
|
|
STATUS |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROSPECTIVE PARENT |
|
|
|
|
DATE |
|
|
|
|
CITY |
|
STATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CURRENT MARRIAGE PLACE |
|
|
|
|
STATUS |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROSPECTIVE PARENT |
|
|
|
|
DATE |
|
|
|
|
CITY |
|
STATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

|
PREVIOUS MARRIAGE INFORMATION |
|
|
||||
|
|
|
|
|
|
|
|
|
PREVIOUS MARRIAGE PLACE |
|
|
HOW TERMINATED |
|||
|
|
|
|
|
|
|
|
PROSPECTIVE PARENT |
|
DATE |
|
CITY |
STATE |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
PREVIOUS MARRIAGE PLACE |
|
|
HOW TERMINATED |
|||
|
|
|
|
|
|
|
|
PROSPECTIVE PARENT |
|
DATE |
|
CITY |
STATE |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
LIST ALL HOUSEHOLD MEMBERS |
|
|||
|
|
|
|
|
|
FULL NAME |
|
DATE OF BIRTH |
RELIGION |
RACE |
RELATIONSHIP |
|
|
MM/DD/YYYY |
|
|
|
1. |
|
|
|
|
Self |
2. |
|
|
|
|
|
3. |
|
|
|
|
|
4. |
|
|
|
|
|
5. |
|
|
|
|
|
6. |
|
|
|
|
|
7. |
|
|
|
|
|
8. |
|
|
|
|
|
NOTE: If your application is rejected or if your application has not been acted upon within six months of filing by the completion of an adoption study, you may request a State administrative hearing. The hearing must be requested within 60 days after the date of rejection or failure to act.
NOTE: At such hearings, you will have the right to be represented by counsel or other representative to produce witnesses and other evidence on your behalf, to request the issuance of subpoenas, to
New York State Office of Children and Family Services
Special Hearings
52 Washington Street, Room 322 North
Rensselaer, New York 12144
NOTE: Social Services Law
NOTE: Social Services Law
NOTE: If you have acknowledged your willingness to adopt a handicapped or
SIGNATURE OF PROSPECTIVE PARENT |
|
DATE |
|
SIGNATURE OF PROSPECTIVE PARENT |
|
DATE |
Note: Applicant should retain copy of application
INSTRUCTIONS FOR COMPLETING
APPLICATION TO ADOPT FORM
PART I: Family Adoption Registry Information: All prospective adoptive parents who express a willingness to adopt handicapped or
Prospective Parent’s Name: The full name (last, first, middle initial) of the prospective adoptive parent(s). It is possible to list a single parent.
Parent’s DOB: Provide the date of birth (MM/DD/YYYY) of the prospective adoptive parent(s).
Parent’s Ethnicity: Enter parent’s ethnicity. Use ethnicity code from coding guide at the bottom of application.
Parent’s Religion: Enter parent’s religion. Use religion code from coding guide at the bottom of application.
Home Address: Provide the street address of the primary residence.
City/Town: Provide the city/town of the primary residence.
County: Provide the county of the primary residence
State: Provide the state of primary residence.
Zip Code: Provide the zip code of primary residence.
Home Telephone: Provide telephone number including area code of primary residence.
Employment Telephone: Provide prospective parent’s employment telephone number including area code at place (s) of employment.
Family Primary and Secondary Language: Enter the code of the family’s primary and secondary language Use language code from the coding guide at the bottom of the application.
Family Pet: Indicate the type of family pet (as appropriate).
Sex: Indicate with an “E” (Either), “M” (Male), “F”(Female) the sex of the child desired.
Age Indicate with an “X” the appropriate age ranges of child(ren) desired. One or more or all age ranges may be selected. The system will only search the age ranges indicated.
Child’s Ethnicity: Enter ethnicity(ies) of the child(ren) prospective adoptive parent(s) is interested in adopting. Use ethnicity code from coding guide at the bottom of the application.
Child’s Primary and Secondary Language: Enter the code of the child’s primary and secondary language. Use primary and secondary language code form the coding guide at the bottom of the application.
Child’s Religion: Enter religion of the child(ren) prospective adoptive parent(s) is interested in adopting. Use religion code from coding guide at the bottom of the application.
Special Needs: Indicate with an “X” in the appropriate field the willingness of prospective adoptive parent(s) to accept a child with special needs. If a disabled child is not desired, leave this section blank. The system will only search to the degree of disability indicated. Please review the following definitions and examples of the categories of child needs and an explanation of the levels of severity. This is a framework intended to assist caseworker’s to assist matching prospective parents with children available for adoption. It is not the standard for determining rate of payment. Social Services districts establish special exceptional rates in accordance with 18 NYCRR 427.6
CATAGORIES OF CHILD NEEDS
Medical/Physical Needs: This category includes children with specific medical/physical needs that may require an additional level of care beyond that normally given at the child’s age level. This category includes children that may display some of the following medical problems that range from acute to chronic and/or terminal illness: a child who experiences respiratory problems ranging from asthma to reactive airway disease or skin conditions that range from eczema to those that require surgical/medical intervention; children with physical disabilities that impair the use of vision, hearing and mobility; and children with neurological problems that range from seizure disorders to different levels of cerebral palsy. This section will include infants that require additional medical intervention as well as some children who have gastrointestinal medical needs, and children who experience a wide range of allergy conditions. Additionally, children with genetically inherited conditions such as Down’s syndrome, Fetal Alcohol Syndrome, Tourettes and sickle cell disease will be included in this section.
Educational/Learning Needs: This category includes children with educational/learning needs ranging from educational support to diagnosed learning disabilities. Examples will include visual/receptive/auditory processing difficulties, dyslexia and educational delays. In addition children may require special educational intervention.
Mental Health Needs: This category includes children with mental/emotional disorders ranging from experiencing
Supervision (PINS), and Juvenile Delinquents. Further examples of mental health needs include those children exhibiting some of the following behaviors
Developmental Delay Needs: This category includes children whose developmental needs range from receptive/ expressive language, fine/gross motor skills, social adaptations, and
EXPLANATION OF MILD, MODERATE AND SEVERE LEVELS
Mild:
Medical/Physical Needs: - Child has a condition(s) which require
Educational/Learning Needs - Child is slightly behind in one or more subjects but attends regular school classes. Child may have some minor learning disabilities.
Mental Health Needs: - Child has a diagnosed condition that may mildly impair their ability to function such as an adjustment or attachments disorder. Child is generally emotionally stable but may be facing a situation (disruption, new foster home) that has created a temporary emotional stress and may be addressed. Child has or has had a problem controlling their behavior, usually associated with a specific incident such as a disruption.
Developmental Needs: - Child has a mild delay in development and may be receiving speech, occupational or physical therapy.
Moderate:
Medical/Physical Needs: - Child that has a moderate level of cerebral palsy, cleft defects which have not yet
been surgically treated, sickle cell disease if severe complications are not present, partial impairment of normal movement, diabetes, heart defects which can be repaired, spina bifida without the most severe complications.
Educational/Learning Needs: - Child is 2 to 3 years behind in subjects and receiving resource room help or other special tutoring aside from being in the regular classroom.
Mental Health Needs: - Children with one of the described conditions requiring on going intervention services and a higher level of supervision and or treatment. Child is experiencing emotionally related problems that may interfere with child’s school performance or interaction with others. Child has a history of acting out causing problems in school and in interpersonal relationships.
Developmental Needs: - Child needs assistance with skills of daily living. Child is receiving early intervention services for significant lags in speech, fine/gross motor skills.
