
The PDF editor was created with the purpose of making it as simple and easy-to-use as it can be. The next steps will help make creating the undersigned easy and quick.
Step 1: Click the orange "Get Form Now" button on the following webpage.
Step 2: Right now, you can start editing the undersigned. The multifunctional toolbar is available to you - add, erase, adjust, highlight, and undertake several other commands with the content material in the form.
The following segments will help make up your PDF file:
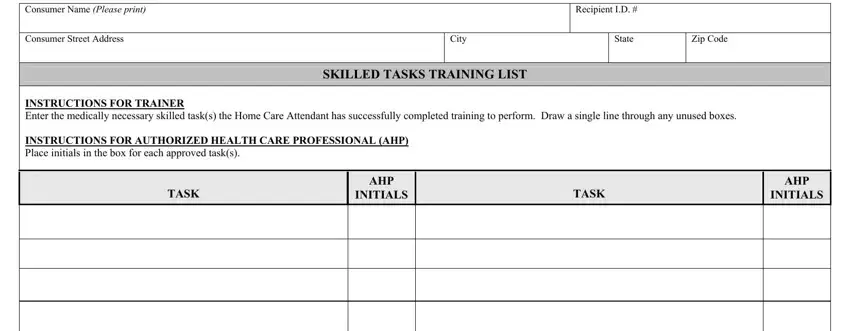
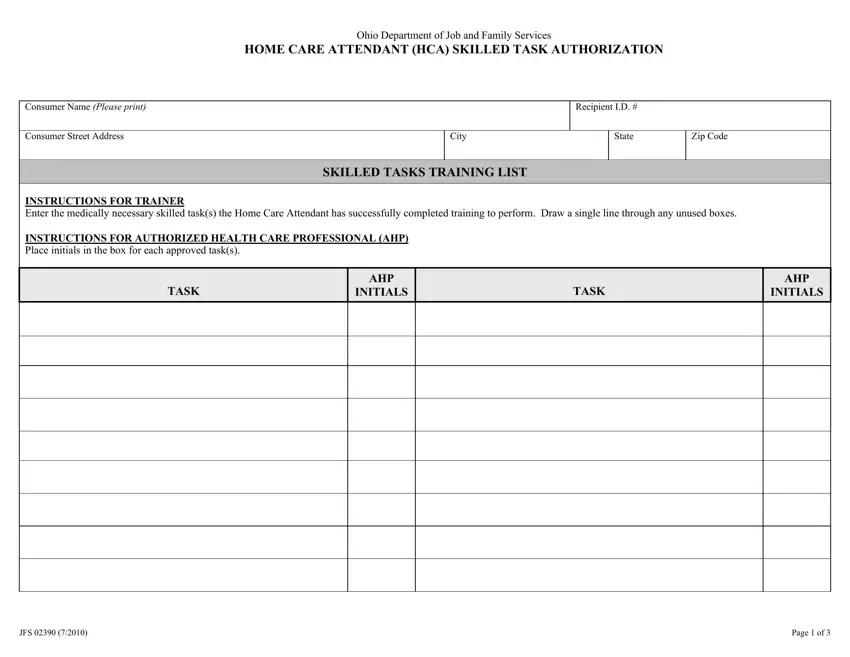
You need to type in the appropriate details in the JFS, and Page of field.
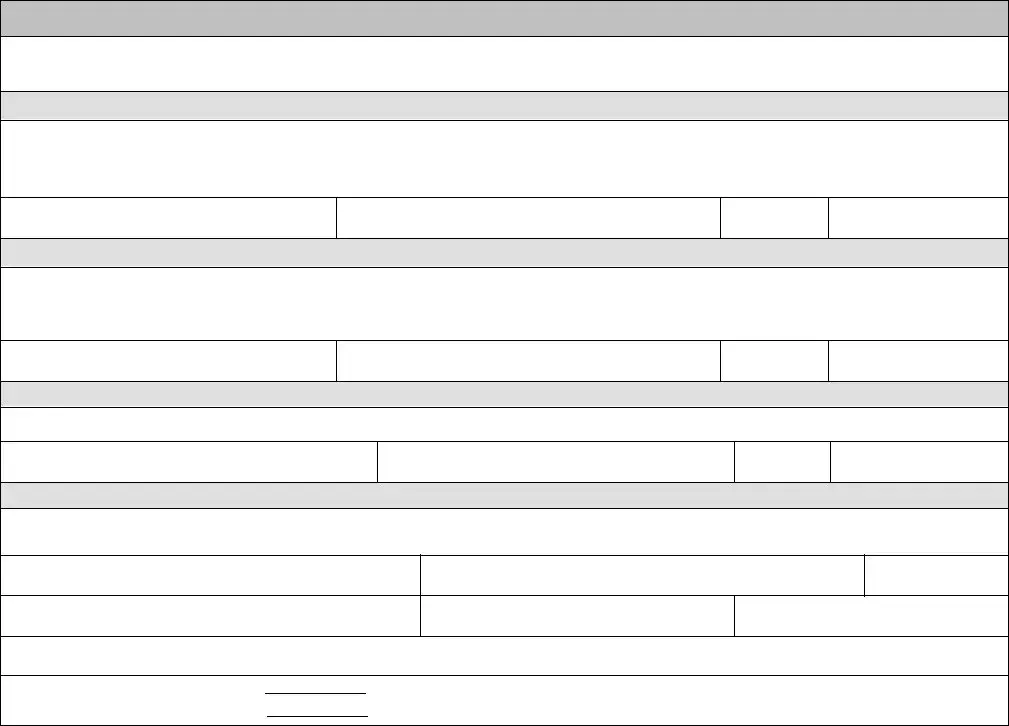
The application will demand for more information with a purpose to instantly complete the part Name Please print, Signature, Initials, Date Signed, HOME CARE ATTENDANT, I the undersigned have received, Name Please print, Signature, Initials, Date Signed, TRAINER Please read before signing, I the undersigned verify that I, Trainer Name Please print, Trainer Signature, and Initials.
Explain the rights and obligations of the sides inside the section Date Signed, Emergency Phone Number Including, Fax Number Including Area Code, In the event that no physician is, CustomerAuthorized Representative, JFS, and Page of.

Finish by reviewing the following sections and filling them in accordingly: Consumer Name Please print, Trainer Name Please print, Effective Period not to exceed, Start Date, End Date, DIRECTIONS Trainer Enter the name, Name of Task, Task Training Detail, and Date Training Completed.
Step 3: Hit the Done button to be certain that your finished file may be exported to any kind of electronic device you prefer or sent to an email you indicate.
Step 4: Come up with no less than a couple of copies of your file to keep away from any kind of potential concerns.
