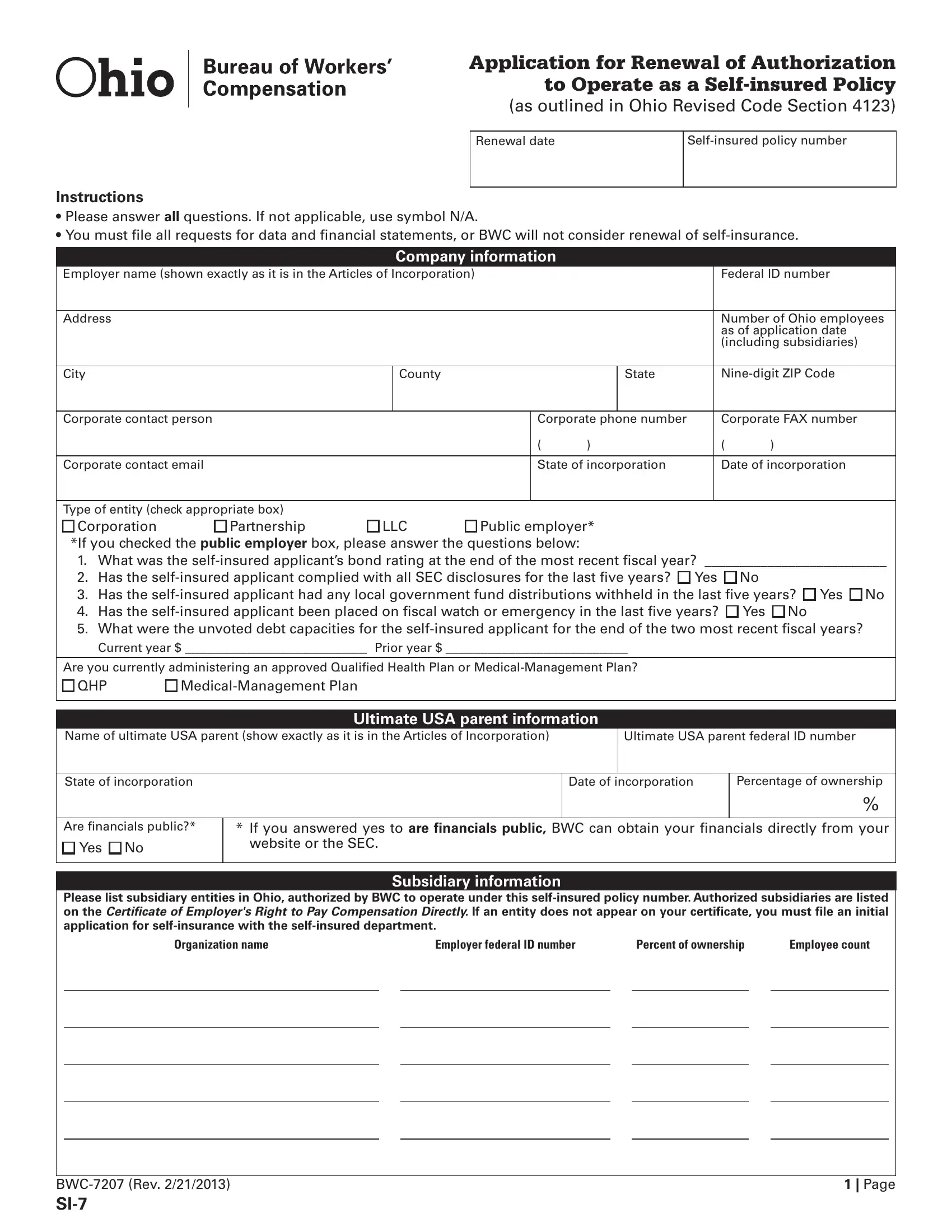
In Ohio, the maintenance and renewal of authorization for companies to operate as self-insured entities for workers' compensation demands attention to a comprehensive application process, outlined in the Ohio Si 7 form. This form serves as a critical tool in aligning with the Ohio Revised Code Section 4123, ensuring that organizations meet specific criteria and obligations to continue their status as self-insured employers. The document requests detailed information from companies, including their basic company information—such as employer name, address, and federal ID number—to more nuanced details about their operations, subsidiaries, and financials. The form delves into specifics, asking for the number of Ohio employees, the type of entity, and details about the ultimate USA parent company. Moreover, it covers compliance aspects, including SEC disclosures and local government fund distributions, alongside financial statements essential for the Bureau of Workers' Compensation (BWC) to consider renewal. Additionally, questions related to corporate restructuring, Ohio administrator changes, and excess workers' compensation insurance illustrate the breadth of data collected to ensure compliance and the ongoing capability of the company to self-insure. Notably, the certification section underscores the legal affirmation of the information's accuracy, verifying the company's commitment to truthful reporting. Furthermore, the form includes sections for claim file housing locations, which highlights the procedural aspect of maintaining and auditing claims records. Through this detailed application process, Ohio upholds the integrity and financial stability of its self-insured workers' compensation system, providing a structured framework for organizations to renew their authorization.
| Question | Answer |
|---|---|
| Form Name | Ohio SI-7 Form |
| Form Length | 8 pages |
| Fillable? | Yes |
| Fillable fields | 361 |
| Avg. time to fill out | 37 min 8 sec |
| Other names | bwc si7, si 7 ohio bwc, ohio wc si 7, ohio si 7 form |