

With the help of the online editor for PDFs by FormsPal, you can easily fill in or change okdhs forms okdhs right here. To retain our editor on the leading edge of efficiency, we aim to put into operation user-oriented capabilities and enhancements regularly. We're always grateful for any suggestions - join us in revolutionizing the way you work with PDF docs. Here is what you'll want to do to start:
Step 1: Hit the orange "Get Form" button above. It's going to open our editor so that you could start filling out your form.
Step 2: With our advanced PDF editing tool, you are able to do more than simply complete blank fields. Express yourself and make your docs seem high-quality with custom textual content added in, or modify the file's original content to perfection - all comes along with the capability to incorporate stunning images and sign the file off.
Pay close attention when filling out this document. Make certain all mandatory blanks are completed properly.
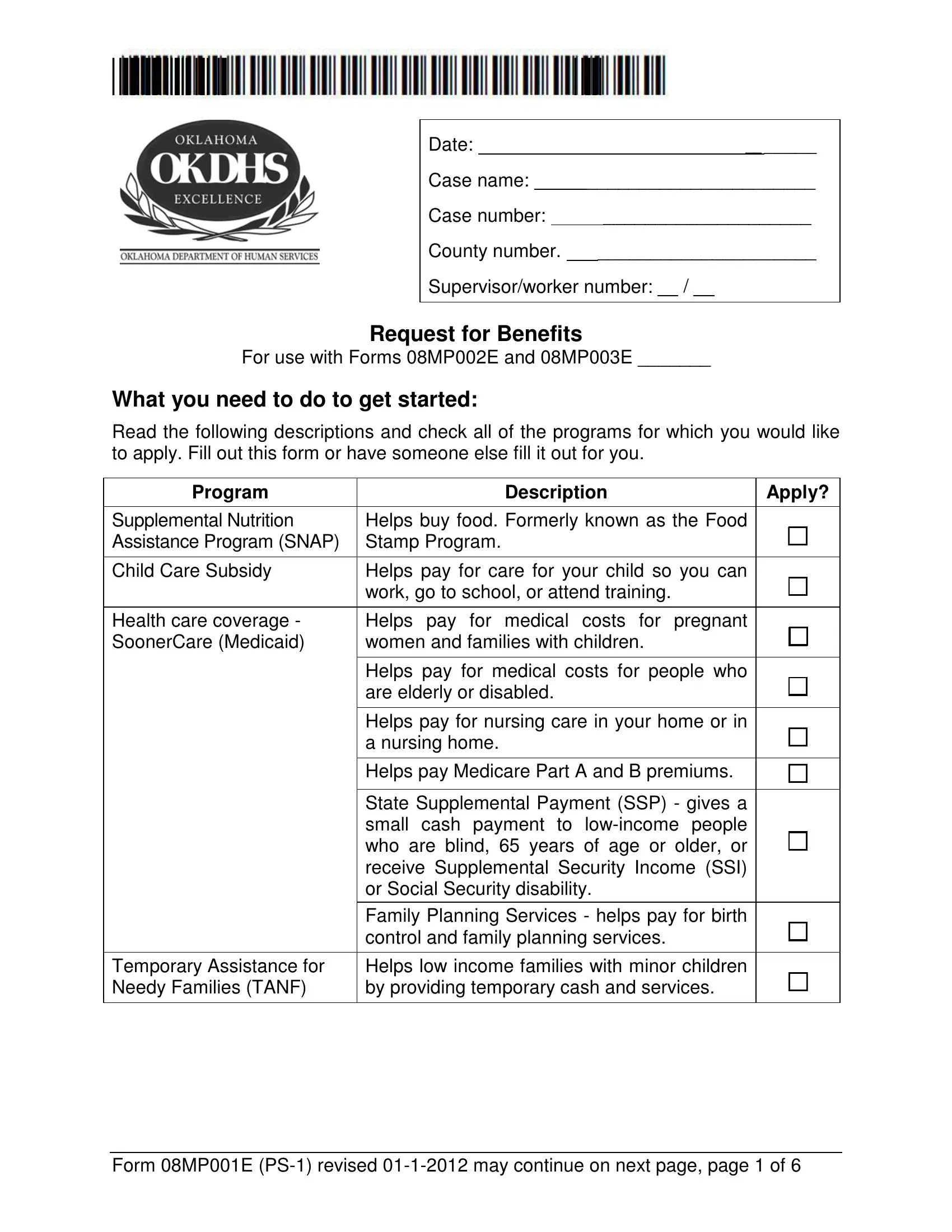
1. The okdhs forms okdhs usually requires specific information to be entered. Make sure the following blanks are finalized:
2. Now that the previous section is completed, you're ready to put in the required particulars in Health care coverage SoonerCare, Temporary Assistance for Needy, Helps pay for medical costs for, Helps pay for medical costs for, Helps pay for nursing care in your, Helps pay Medicare Part A and B, State Supplemental Payment SSP, and Helps low income families with allowing you to move on further.
Be extremely mindful while filling out Temporary Assistance for Needy and Helps pay for nursing care in your, since this is the section where most users make some mistakes.
3. This third stage is usually simple - complete all the empty fields in Monday, Tuesday Wednesday, Thursday, Friday, Morning Afternoon, What you will need to bring to, proof of identity such as driver, name of the place you want to use, You may be asked to give more, How can we contact you, and Name Mailing address street or PO in order to complete this process.
4. The subsequent section requires your attention in the following parts: Name Mailing address street or PO, Email address, State Zip, City, Form MPE PS revised may continue, and page of. Always fill in all requested information to move further.
5. As you come near to the completion of your file, you'll find a few more requirements that should be satisfied. Particularly, Date of birth, Sex M State of birth County of, Person Name of adult head of, Social Security number, American Indian or Alaskan native, Black or African American, Asian, Date of birth, Sex M State of birth County of, and Person Name Name at birth if must be filled in.
Step 3: After looking through the fields you've filled in, hit "Done" and you are good to go! Right after getting a7-day free trial account at FormsPal, you'll be able to download okdhs forms okdhs or send it via email promptly. The PDF document will also be accessible from your personal cabinet with your each change. We don't share the information that you enter whenever filling out documents at FormsPal.