Do you have an OMRF Form DC 4 10 to complete? Do not panic! A common legal document in the medical field, this form is required in order to give out certain types of health care services and products. In this blog article, we will go through the purpose of this important form and provide helpful tips on how to properly fill it out accurately and quickly while avoiding any costly missteps down the line. Keep reading if you're feeling a bit lost trying to come up with all that information - we'll help get your ready for submission in no time!
| Question | Answer |
|---|---|
| Form Name | Omrf Form Dc 4 10 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | taxable, Oklahoma, withholdings, deducted |
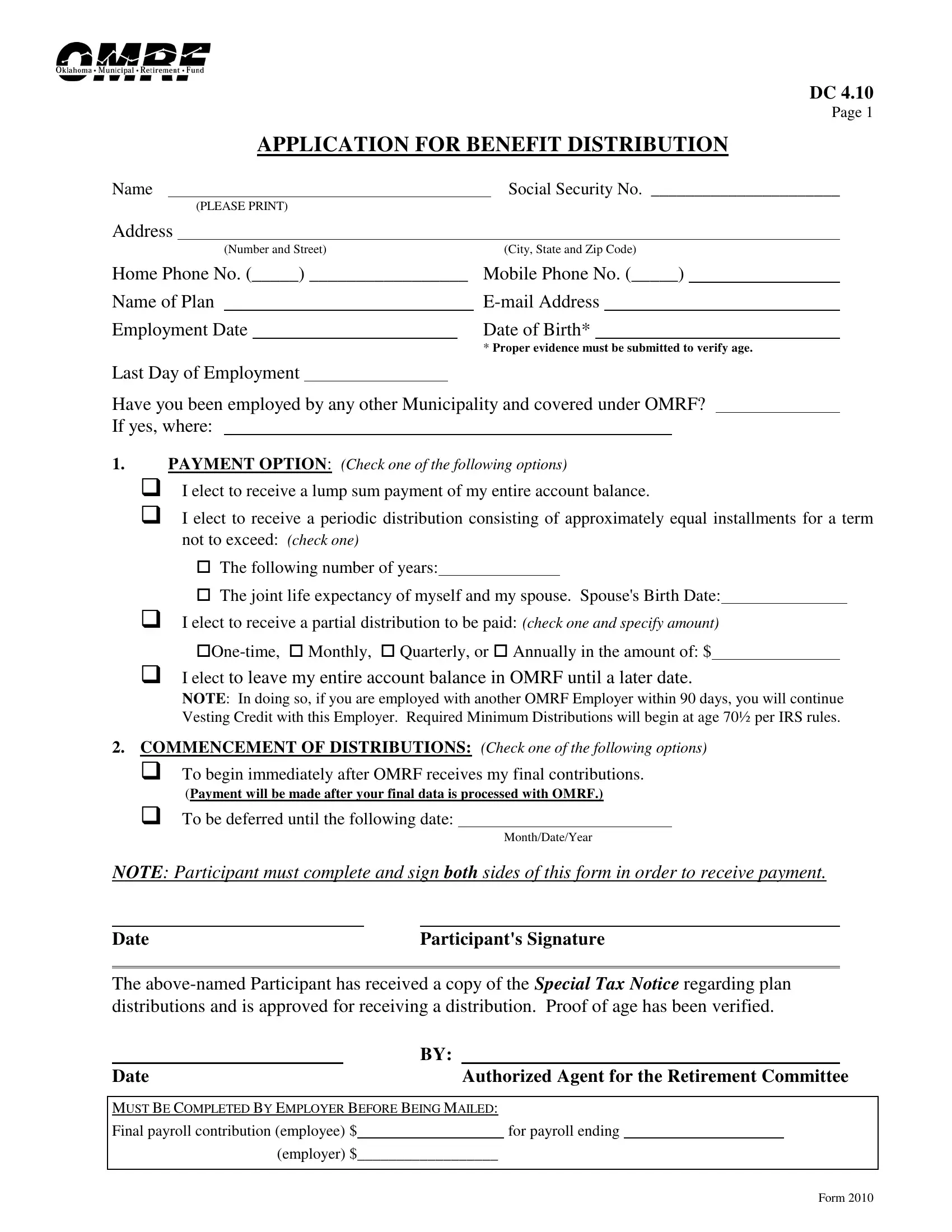
DC 4.10
Page 1
APPLICATION FOR BENEFIT DISTRIBUTION
Name |
|
Social Security No. ______________________ |
|
(PLEASE PRINT) |
|
Address
|
(Number and Street) |
(City, State and Zip Code) |
|||||
Home Phone No. (_____) _________________ |
Mobile Phone No. (_____) |
|
|||||
Name of Plan |
|
|
|||||
Employment Date |
|
|
Date of Birth* |
|
|||
|
|
|
|
* Proper evidence must be submitted to verify age. |
|||
Last Day of Employment
Have you been employed by any other Municipality and covered under OMRF? If yes, where:
1.PAYMENT OPTION: (Check one of the following options)
I elect to receive a lump sum payment of my entire account balance.
I elect to receive a periodic distribution consisting of approximately equal installments for a term not to exceed: (check one)
The following number of years:
The joint life expectancy of myself and my spouse. Spouse's Birth Date:
I elect to receive a partial distribution to be paid: (check one and specify amount)
I elect to leave my entire account balance in OMRF until a later date.
NOTE: In doing so, if you are employed with another OMRF Employer within 90 days, you will continue Vesting Credit with this Employer. Required Minimum Distributions will begin at age 70½ per IRS rules.
2.COMMENCEMENT OF DISTRIBUTIONS: (Check one of the following options)
To begin immediately after OMRF receives my final contributions.
|
(Payment will be made after your final data is processed with OMRF.) |
||||
To be deferred until the following date: |
|
|
|||
|
|
|
|
Month/Date/Year |
|
NOTE: Participant must complete and sign both sides of this form in order to receive payment. |
|||||
|
|
|
|
||
Date |
|
|
Participant's Signature |
||
The
|
|
|
BY: |
|
|
|||
Date |
|
Authorized Agent for the Retirement Committee |
||||||
|
|
|
|
|||||
MUST BE COMPLETED BY EMPLOYER BEFORE BEING MAILED: |
||||||||
Final payroll contribution (employee) $ |
|
|
for payroll ending |
|||||
|
(employer) $ |
__________________ |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
Form 2010

DC 4.10
Page 2
TAX WITHHOLDING ELECTION
Federal and State Income Tax Withholding
Name |
|
|
Social Security No. |
|
|
COMPLETE SECTION “A” OR “B” BELOW: |
Name of Plan |
|
|||
Section A. RECURRING PAYMENTS (monthly) – Federal and State Income Tax Withholding
Instructions: As a benefit recipient, the following withholding alternatives are available to you:
You may specify that you do not want any federal or state income tax deducted from your benefit by selecting No. 1 below.
You may elect to use withholding tax tables by selecting No. 2 below and completing the marital status and number of allowances which will require the OMRF system to determine the amount, if any, which must be withheld based on federal and state withholding tables. If elected, the tax withholdings may or may not meet your required amounts.
You may elect to withhold a specified percentage or amount for federal and state income taxes by selecting No. 3 below.
In requesting the distribution of my funds from OMRF, I designate the following withholding election. This election will remain in effect until I submit another Tax Withholding Election.
1. |
_______ |
I elect not to have Federal or State income tax withheld. |
|||
2. |
_______ |
I wish to have OMRF withhold from my monthly benefit the amount of federal and state income tax |
|||
|
|
as determined in accordance with withholding tax tables and the allowances claimed below: |
|||
|
|
Single Married |
Married |
||
|
|
_____ Number of withholding allowances/exemptions you want to claim. |
|||
3. |
a. _______ |
I wish to have |
|
|
(% or $ amount) of Federal income tax withheld. |
|
b. _______ |
I wish to have |
|
|
(% or $ amount) of State income tax withheld. |
If you do not file a Tax Withholding Election form with OMRF, we are required by law to assume that you are married and are claiming 3 (three) allowances. We will automatically withhold federal and state income tax if your payment is large enough to require withholdings.
Section B.
Instructions: When receiving a total (or
The distribution can be made payable to you directly, in which case a mandatory 20% Federal tax withholding and an optional 5% Oklahoma state tax withholding will occur. (The mandatory tax withholding only applies to the taxable portion of your distribution.) OR
You can direct OMRF to roll over the distribution into an IRA or other qualified plan without taxes being withheld. You
will receive the
distributions are mailed directly to your address of record.
In requesting the distribution of my funds from OMRF, I designate the following method of payment:
1.a. _____ I WANT THE CHECK(S) MADE PAYABLE TO ME. I am aware of the mandatory 20% Federal tax withholding on the taxable portion of my distribution.
(If one of the following is not selected, Oklahoma taxes will be withheld from the distribution.)
b. _____ I do NOT want Oklahoma State income tax withheld from the taxable part of my distribution.
c. _____ I do want Oklahoma State income tax withheld from the taxable part of my distribution.
(Withholding rate is 5% and is subject to change based on State withholding tables.)
2._______ I WANT A DIRECT ROLLOVER TO A TRADITIONAL IRA. (YOU MUST SUBMIT A COPY OF YOUR IRA AGREEMENT FOR A DIRECT ROLLOVER.)
3._______ I WANT A DIRECT ROLLOVER TO A QUALIFIED PLAN. (YOU MUST SUBMIT A COPY OF A RECENT PARTICIPANT STATEMENT AND THE PLAN’S CONTACT INFORMATION.)
I have reviewed the information above and hereby submit this statement of preference regarding how my benefit distribution is to be treated for purposes of federal and state income tax withholding.
Date |
|
Participant’s Signature |
Form 2010