
Once you open the online PDF editor by FormsPal, you are able to fill in or alter va form 10 1394 pdf here. Our tool is continually developing to provide the best user experience attainable, and that's due to our resolve for continuous enhancement and listening closely to comments from users. All it requires is a few basic steps:
Step 1: Access the PDF form in our editor by pressing the "Get Form Button" above on this webpage.
Step 2: As soon as you access the editor, you will get the document ready to be filled in. Other than filling in different fields, you can also do some other things with the PDF, such as adding your own text, changing the initial textual content, inserting images, affixing your signature to the document, and more.
Completing this PDF needs care for details. Make certain each blank field is filled out properly.
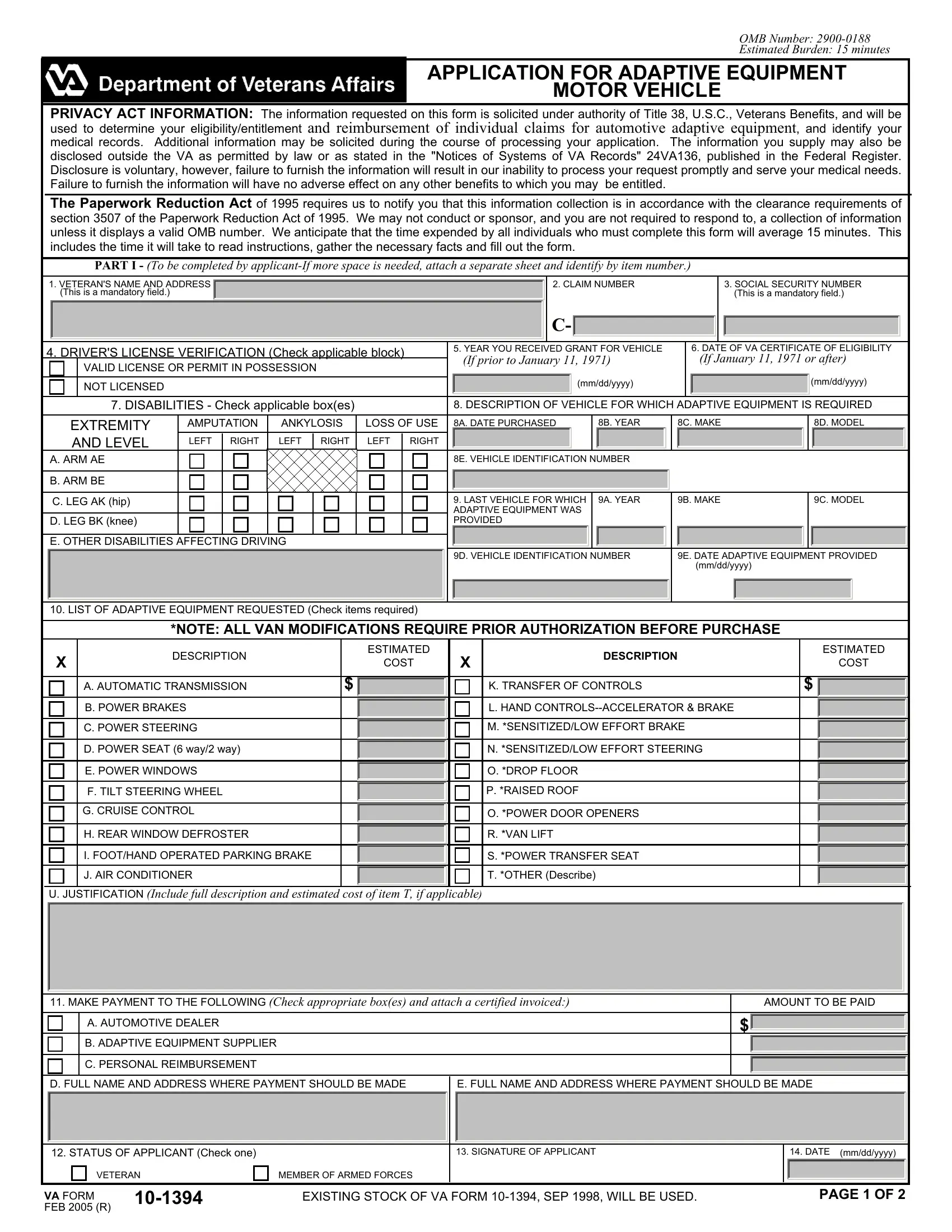
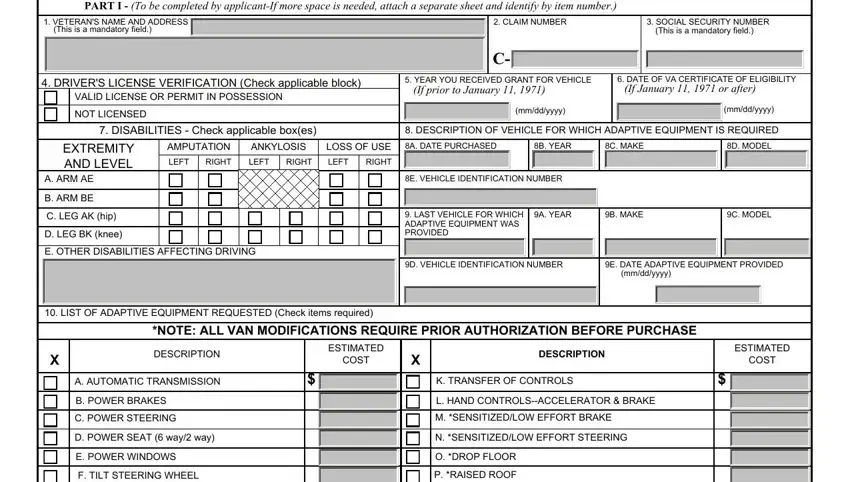
1. Whenever completing the va form 10 1394 pdf, make certain to complete all important blanks within its associated form section. This will help to speed up the process, allowing for your details to be handled swiftly and correctly.
2. After this section is done, you're ready put in the needed details in G CRUISE CONTROL, H REAR WINDOW DEFROSTER, I FOOTHAND OPERATED PARKING BRAKE, J AIR CONDITIONER, O POWER DOOR OPENERS, R VAN LIFT, S POWER TRANSFER SEAT, T OTHER Describe, U JUSTIFICATION Include full, MAKE PAYMENT TO THE FOLLOWING, AMOUNT TO BE PAID, A AUTOMOTIVE DEALER, B ADAPTIVE EQUIPMENT SUPPLIER, C PERSONAL REIMBURSEMENT, and D FULL NAME AND ADDRESS WHERE so you're able to move on further.
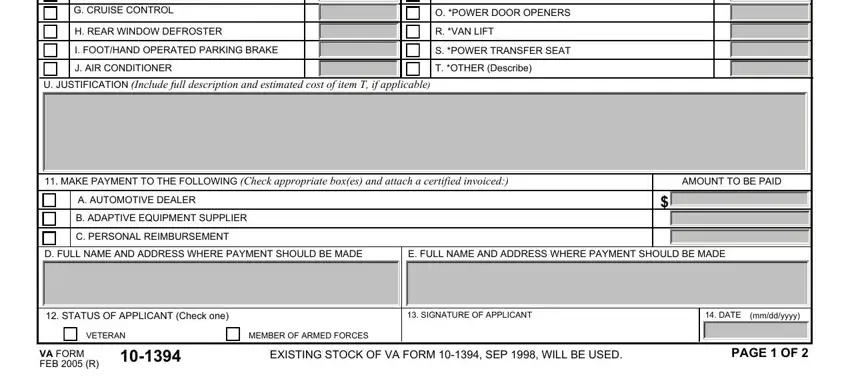
It is easy to make an error when completing your H REAR WINDOW DEFROSTER, and so be sure to go through it again before you send it in.
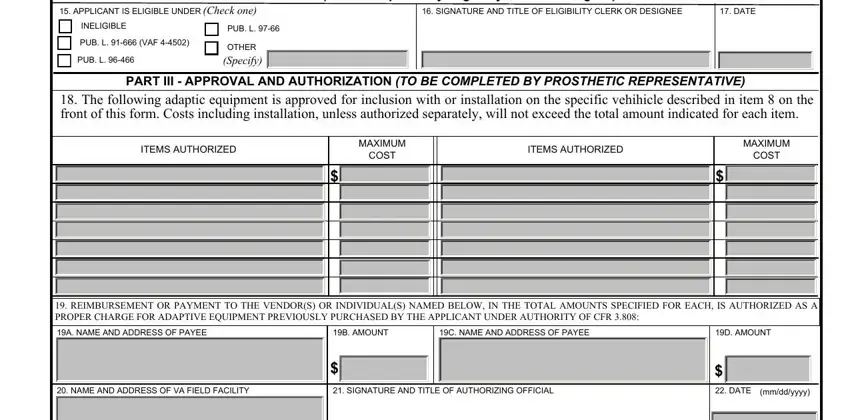
3. In this particular step, take a look at PART II ELIGIBILITY To be, APPLICANT IS ELIGIBLE UNDER Check, INELIGIBLE, PUB L VAF, PUB L, PUB L, OTHER Specify, SIGNATURE AND TITLE OF, DATE, PART III APPROVAL AND, The following adaptic equipment, ITEMS AUTHORIZED, MAXIMUM, COST, and ITEMS AUTHORIZED. Each of these will have to be filled in with highest precision.
4. All set to begin working on the next segment! Here you'll have these PART IV CERTIFICATION OF RECEIPT, I CERTIFY THAT I have received the, SIGNATURE OF APPLICANT, DATE, mmddyyyy, INSTRUCTIONS TO VETERAN OR, Contact should be made with the, If you are requesting adaptive, After approval you may give the, In the event you must obtain some, After receipt of the items or, INSTRUCTIONS TO SELLERVENDOR, This is to inform you that if, After you and the applicant have, and I certify that the amounts billed blank fields to fill in.
5. To conclude your form, the particular area involves some additional blank fields. Filling out I certify that the amounts billed, Signature of Company Official, Attach copies of VA Form or, VA FORM FEB R, and PAGE of will conclude the process and you're going to be done very quickly!

Step 3: Before finishing your form, ensure that all blanks are filled out correctly. As soon as you confirm that it's good, click “Done." Get your va form 10 1394 pdf the instant you join for a free trial. Immediately gain access to the pdf form in your personal cabinet, together with any modifications and changes conveniently kept! At FormsPal.com, we do everything we can to ensure that all of your information is stored protected.