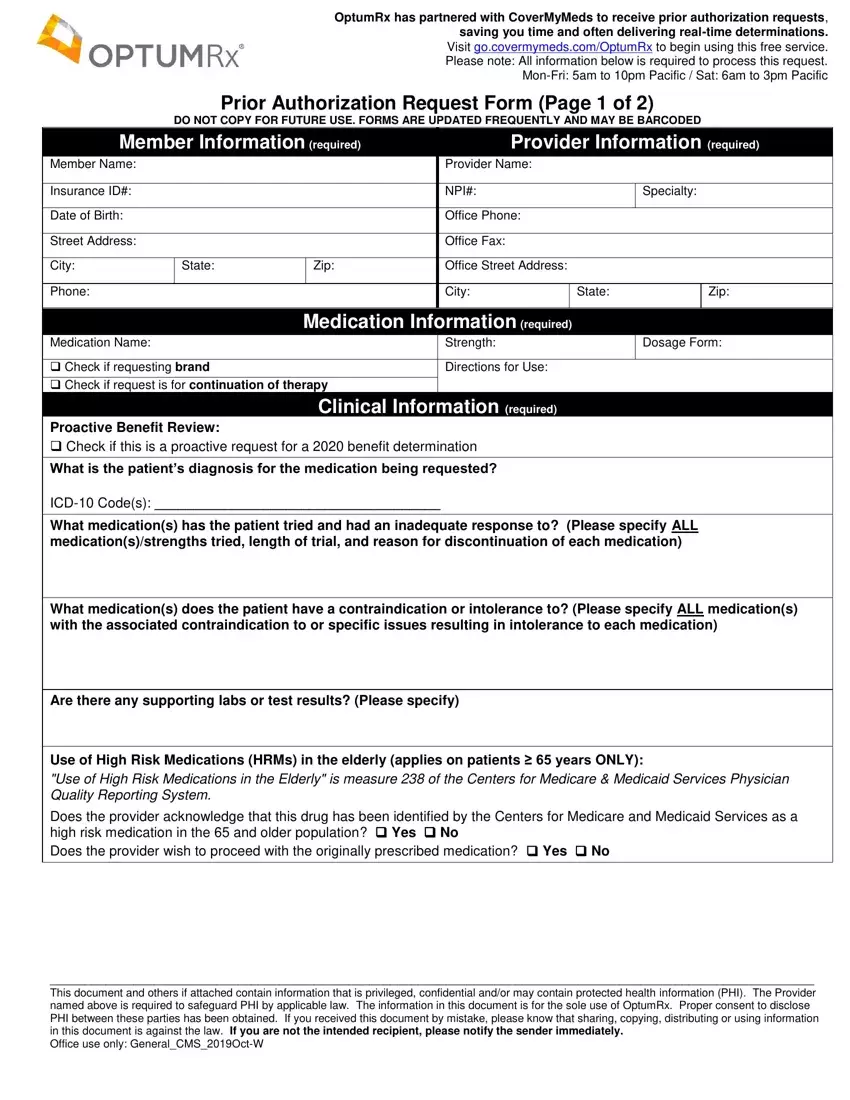
OptumRx has partnered with CoverMyMeds to receive prior authorization requests, saving you time and often delivering real-time determinations.
Visit go.covermymeds.com/OptumRx to begin using this free service.
Please note: All information below is required to process this request.
Mon-Fri: 5am to 10pm Pacific / Sat: 6am to 3pm Pacific
Prior Authorization Request Form (Page 1 of 2)
DO NOT COPY FOR FUTURE USE. FORMS ARE UPDATED FREQUENTLY AND MAY BE BARCODED
|
Member Information (required) |
|
|
Provider Information (required) |
|
|
|
|
|
|
Member Name: |
|
|
|
|
|
Provider Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance ID#: |
|
|
|
|
|
NPI#: |
|
Specialty: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Birth: |
|
|
|
|
|
Office Phone: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address: |
|
|
|
|
|
Office Fax: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
State: |
|
Zip: |
|
Office Street Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
|
|
City: |
|
State: |
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Medication Information (required) |
|
|
|
|
|
Medication Name: |
|
|
|
|
|
Strength: |
|
Dosage Form: |
|
|
|
|
|
|
|
|
|
|
|
|
Check if requesting brand |
|
|
|
|
Directions for Use: |
|
|
|
|
|
Check if request is for continuation of therapy |
|
|
|
|
|
|
|
|
|
|
|
Clinical Information (required) |
|
|
|
|
|
Proactive Benefit Review: |
|
|
|
|
|
|
|
|
|
|
|
Check if this is a proactive request for a 2020 benefit determination |
|
|
|
|
|
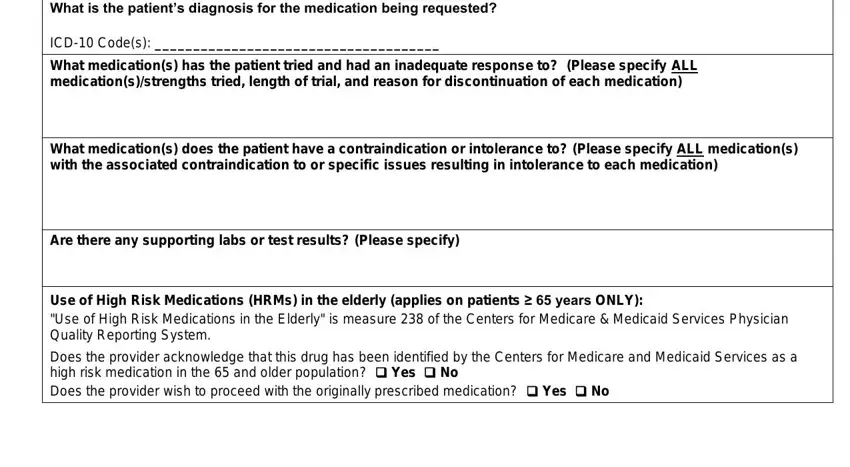
What is the patient’s diagnosis for the medication being requested? |
|
|
|
|
ICD-10 Code(s): _____________________________________
What medication(s) has the patient tried and had an inadequate response to? (Please specify ALL medication(s)/strengths tried, length of trial, and reason for discontinuation of each medication)
What medication(s) does the patient have a contraindication or intolerance to? (Please specify ALL medication(s) with the associated contraindication to or specific issues resulting in intolerance to each medication)
Are there any supporting labs or test results? (Please specify)
Use of High Risk Medications (HRMs) in the elderly (applies on patients ≥ 65 years ONLY):
"Use of High Risk Medications in the Elderly" is measure 238 of the Centers for Medicare & Medicaid Services Physician Quality Reporting System.
Does the provider acknowledge that this drug has been identified by the Centers for Medicare and Medicaid Services as a high risk medication in the 65 and older population? Yes No
Does the provider wish to proceed with the originally prescribed medication? Yes No
______________________________________________________________________________________________________________
This document and others if attached contain information that is privileged, confidential and/or may contain protected health information (PHI). The Provider named above is required to safeguard PHI by applicable law. The information in this document is for the sole use of OptumRx. Proper consent to disclose PHI between these parties has been obtained. If you received this document by mistake, please know that sharing, copying, distributing or using information in this document is against the law. If you are not the intended recipient, please notify the sender immediately.
Office use only: General_CMS_2019Oct-W
Prior Authorization Request Form (Page 2 of 2)
DO NOT COPY FOR FUTURE USE. FORMS ARE UPDATED FREQUENTLY AND MAY BE BARCODED
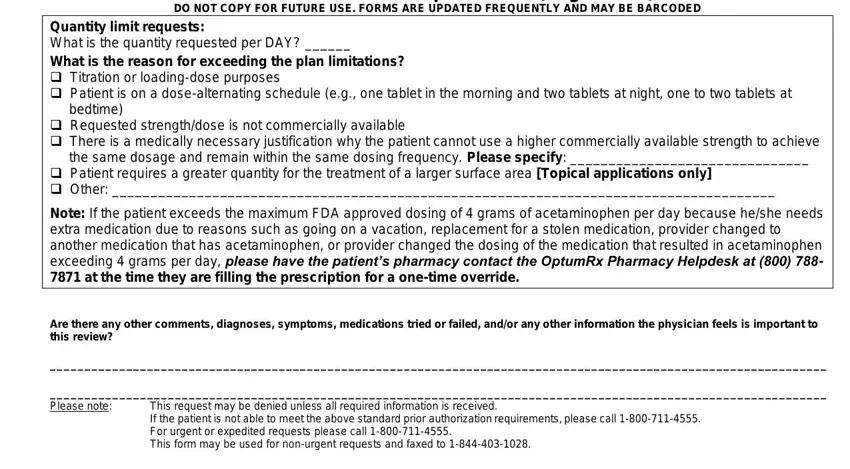
Quantity limit requests:
What is the quantity requested per DAY? ______
What is the reason for exceeding the plan limitations?
Titration or loading-dose purposes
Patient is on a dose-alternating schedule (e.g., one tablet in the morning and two tablets at night, one to two tablets at bedtime)
Requested strength/dose is not commercially available
There is a medically necessary justification why the patient cannot use a higher commercially available strength to achieve the same dosage and remain within the same dosing frequency. Please specify: _______________________________
Patient requires a greater quantity for the treatment of a larger surface area [Topical applications only]
Other: ______________________________________________________________________________________
Note: If the patient exceeds the maximum FDA approved dosing of 4 grams of acetaminophen per day because he/she needs extra medication due to reasons such as going on a vacation, replacement for a stolen medication, provider changed to another medication that has acetaminophen, or provider changed the dosing of the medication that resulted in acetaminophen exceeding 4 grams per day, please have the patient’s pharmacy contact the OptumRx Pharmacy Helpdesk at (800) 788- 7871 at the time they are filling the prescription for a one-time override.
Are there any other comments, diagnoses, symptoms, medications tried or failed, and/or any other information the physician feels is important to this review?
________________________________________________________________________________________________________________
________________________________________________________________________________________________________________
Please note: This request may be denied unless all required information is received.
If the patient is not able to meet the above standard prior authorization requirements, please call 1-800-711-4555. For urgent or expedited requests please call 1-800-711-4555.
This form may be used for non-urgent requests and faxed to 1-844-403-1028.
______________________________________________________________________________________________________________
This document and others if attached contain information that is privileged, confidential and/or may contain protected health information (PHI). The Provider named above is required to safeguard PHI by applicable law. The information in this document is for the sole use of OptumRx. Proper consent to disclose PHI between these parties has been obtained. If you received this document by mistake, please know that sharing, copying, distributing or using information in this document is against the law. If you are not the intended recipient, please notify the sender immediately.
Office use only: General_CMS_2019Oct-W