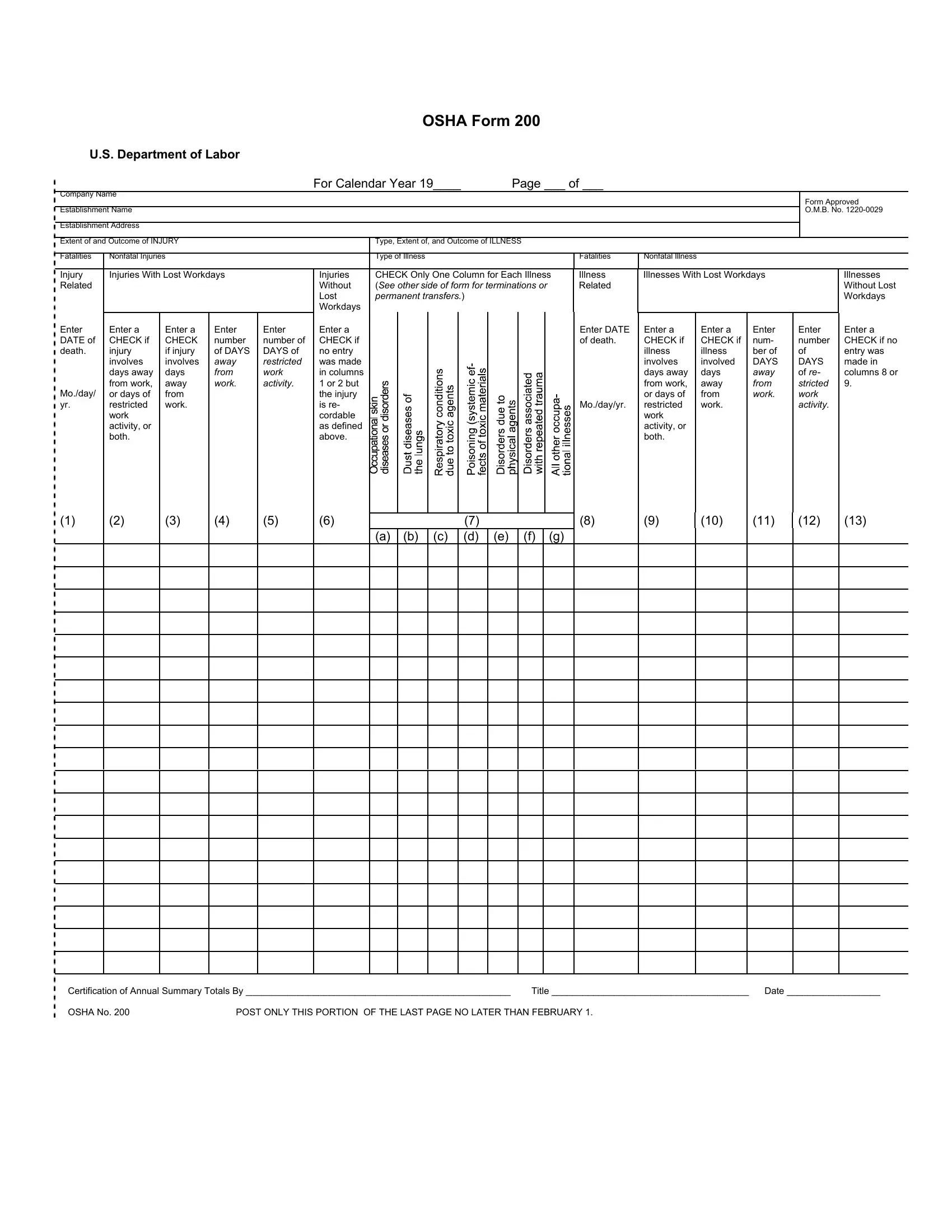
The OSHA Form 200, endorsed by the U.S. Department of Labor, operates as a crucial tool in the realm of occupational safety and health documentation for the calendar year it covers. At its core, the form serves as a comprehensive log and summary of occupational injuries and illnesses, which businesses are mandated to maintain and post within their establishments. This record-keeping not only aids in monitoring workplace safety incidents but also plays a vital role in the formulation of preventive measures against future occurrences. It meticulously categorizes incidents into injuries and illnesses, delineating between fatal and nonfatal outcomes, and further specifies cases involving lost workdays. Moreover, this form demands detailed entry of each incident, including the date, employee details, a description of the injury or illness alongside its extent, and the outcome. By requiring information about days away from work or days of restricted activity, it facilitates an in-depth analysis of the impact of workplace incidents. The obligation to complete and publicly post the summary of this form by a set deadline underscores the importance of transparency and accountability in upholding workplace safety. With penalties for noncompliance, the OSHA Form 200 exemplifies a rigorous approach towards ensuring that occupational health standards are not just met but continuously improved upon.
| Question | Answer |
|---|---|
| Form Name | Osha 200 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | osha log 200 form, osha form 200 log, osha form 200, osha 200 logs |
OSHA Form 200
U.S. Department of Labor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
For Calendar Year 19____ |
|
|
|
Page ___ of ___ |
|
|
|
|
|
|
|
|||||||||||||||
Company Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form Approved |
|
Establishment Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O.M.B. No. |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Establishment Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Extent of and Outcome of INJURY |
|
|
|
Type, Extent of, and Outcome of ILLNESS |
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fatalities |
Nonfatal Injuries |
|
|
|
Type of Illness |
|
|
|
|
|
|
|
|
|
|
|
Fatalities |
Nonfatal Illness |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Injury |
Injuries With Lost Workdays |
|
Injuries |
CHECK Only One Column for Each Illness |
Illness |
Illnesses With Lost Workdays |
|
|
Illnesses |
||||||||||||||||||||||
Related |
|
|
|
|
Without |
(See other side of form for terminations or |
Related |
|
|
|
|
|
|
Without Lost |
|||||||||||||||||
|
|
|
|
|
Lost |
permanent transfers.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Workdays |
||||||
|
|
|
|
|
Workdays |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter |
Enter a |
Enter a |
Enter |
Enter |
Enter a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter DATE |
Enter a |
|
Enter a |
Enter |
Enter |
Enter a |
|
DATE of |
CHECK if |
CHECK |
number |
number of |
CHECK if |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of death. |
CHECK if |
|
CHECK if |
num- |
number |
CHECK if no |
|
death. |
injury |
if injury |
of DAYS |
DAYS of |
no entry |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
illness |
|
illness |
ber of |
of |
entry was |
|
|
involves |
involves |
away |
restricted |
was made |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
involves |
|
involved |
DAYS |
DAYS |
made in |
|
|
days away |
days |
from |
work |
in columns |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
days away |
|
days |
away |
of re- |
columns 8 or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
from work, |
away |
work. |
activity. |
1 or 2 but |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
from work, |
|
away |
from |
stricted |
9. |
|
Mo./day/ |
or days of |
from |
|
|
the injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or days of |
|
from |
work. |
work |
|
|
yr. |
restricted |
work. |
|
|
is re- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mo./day/yr. |
restricted |
|
work. |
|
activity. |
|
|
|
work |
|
|
|
cordable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
work |
|
|
|
|
|
|
|
activity, or |
|
|
|
as defined |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
activity, or |
|
|
|
|
|
|
|
both. |
|
|
|
above. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
both. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(a) (b) (c) (d) (e) (f) (g)
(8)
(9)
(10)
(11) (12) (13)
Certification of Annual Summary Totals By ___________________________________________________ |
Title ______________________________________ Date __________________ |
|
OSHA No. 200 |
POST ONLY THIS PORTION OF THE LAST PAGE NO LATER THAN FEBRUARY 1. |
|

Bureau of Labor Statistics
Log and Summary of Occupational
Injuries and Illnesses
NOTE: This form is required by Public Law |
|
RECORDABLE CASES: You are required to record information about every |
|||||
must be kept in the establishment for 5 years. |
|
occupational death, every nonfatal occupational illness, and those nonfatal |
|||||
Failure to maintain and post can result in the |
|
occupational injuries which involve one or more of the following: loss of |
|||||
issuance of citations and assessments of penalties. |
|
consciousness, restriction of work or motion, transfer to another job, or medical |
|||||
(See posting requirements on the other side of |
|
treatment (other than first aid). (See definitions on the other side of form.) |
|||||
form.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Case or |
Date of |
Employee’s Name |
Occupation |
|
Department |
Description of Injury or Illness |
|
File |
Injury or |
|
|
|
|
|
|
Number |
Onset of |
|
|
|
|
|
|
|
Illness |
|
|
|
|
|
|
Enter a |
Enter |
Enter first name or |
Enter regular job |
Enter department in |
Enter a brief description of the injury or illness and |
||
nondupli- |
Mo./day. |
initial, middle initial, |
title, not activity |
which the employee |
indicate the part or parts of body affected. |
||
cating |
|
last name. |
employee was |
is regularly |
|
||
number |
|
|
performing when |
employed or a |
|
||
which will |
|
|
injured or at |
|
description of normal |
|
|
facilitate |
|
|
onset of illness. |
workplace to which |
|
||
com- |
|
|
In the absence of |
employee is |
Typical entries for this column might be: Amputation of |
||
parisons |
|
|
a formal title, |
|
assigned, even |
1st joint right forefinger; Strain of lower back; Contact |
|
with |
|
|
enter a brief |
|
thought temporarily |
dermatitis on both hands; |
|
supple- |
|
|
description of the |
working in another |
|
||
mentary |
|
|
employee’s |
|
department at the |
|
|
records. |
|
|
duties. |
|
time of the injury or |
|
|
|
|
|
|
|
|
illness |
|
(A) |
(B) |
(C) |
(D) |
|
(E) |
(F) |
|
|
|
|
|
|
|
|
PREVIOUS PAGE TOTALS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTALS (Instructions on other side of form) |
|
|
|
|
|
|
|
|