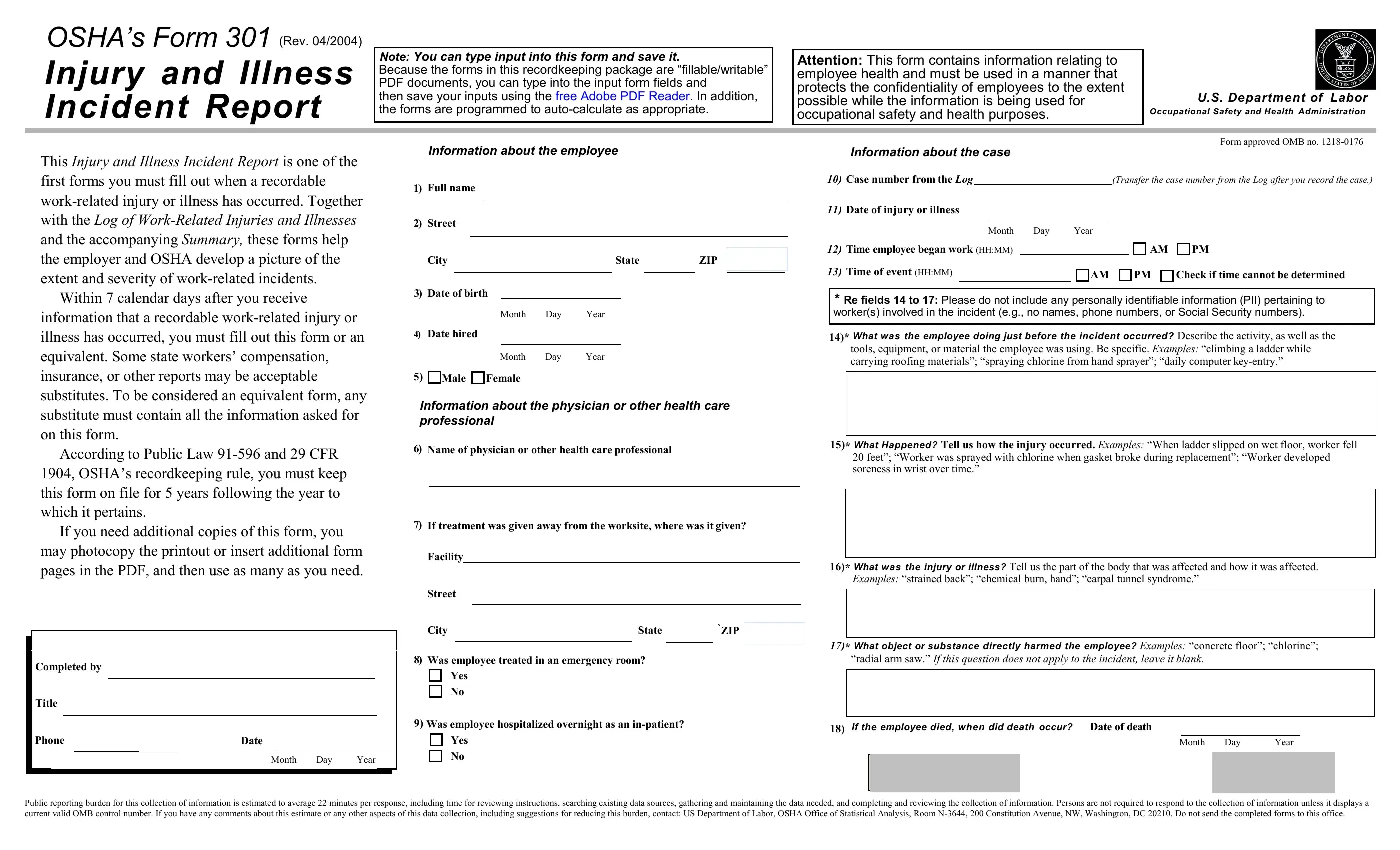
Employers must complete this form, or an equivalent, within 7 calendar days of learning about a recordable incident. This form is integral to workplace safety management, helping employers and OSHA track incidents to assess workplace safety and compliance with regulations.
The main information captured on the OSHA Form 301 includes:
- Details about the injured or ill employee (e.g., name, date of birth, employment date).
- A description of the incident, including what the employee was doing at the time, the exact nature of the injury or illness, and any equipment involved.
- Information about the medical treatment received and the healthcare provider involved.
This form documents the incident for compliance and monitoring and is used as a preventive measure to aid in identifying hazardous conditions. Adhering to the requirements of maintaining and updating these records and keeping them stored for 5 years after they are relevant helps develop strategies to improve workplace safety.
| Question | Answer |
|---|---|
| Form Name | OSHA Form 301 |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 18 |
| Avg. time to fill out | 10 min |
| Other names | OSHA form 301, form OSHA, OSHA accident report form, OSHA form 301 printable |