INSTRUCTIONS
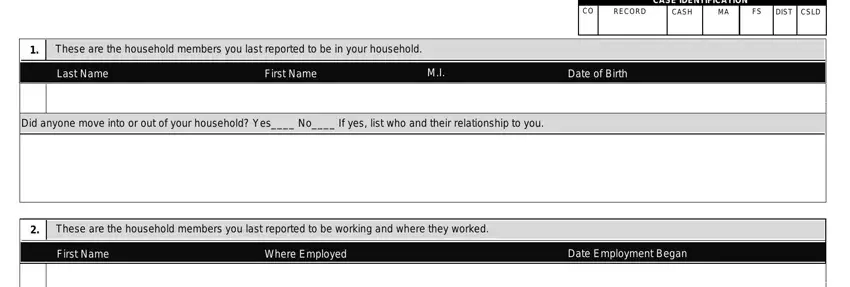
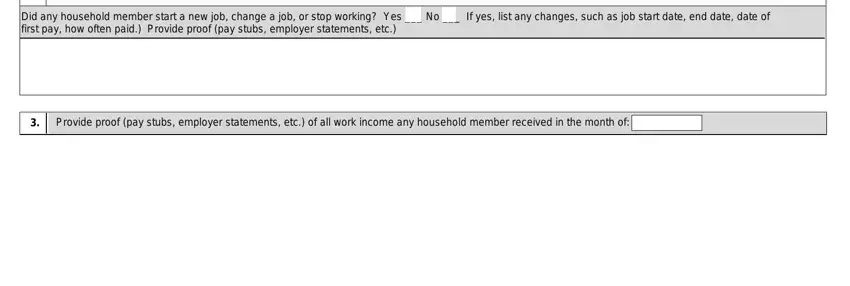
Your household circumstances require you to report semiannually (every 6 months). The information on the semiannual reporting form is needed to determine your continued eligibility for cash, food stamps, Extended Medical Coverage and/or Medicaid. It is also needed to calculate the amount of your monthly cash and/or food stamp benefits. You must give us information for the reporting month shown on page 1 of the form. You are asked to provide child care information: failure to do so could lead to lower benefits or ineligibility.
Note: You may report changes at any time if the change would increase your benefits (such as if you lose your job or your hours of work decrease).
When answering the questions, you must give us information for all persons included in your cash, food stamps and/or Medicaid benefits. This includes stepparents and information for sponsors of aliens, even if the sponsor does not live in your home. You can use a separate sheet of paper to explain any of your answers or give additional information. A separate sheet of paper must be sent in with the form.
You must complete, sign and return the form to the county assistance office by the date shown on page 1 of the form. IF YOU NEED HELP TO COMPLETE THE.FORM, CALL YOUR CASEWORKER OR CHANGE CENTER.
. NOTICE
.If the form is late or incomplete, you may not receive you cash and/or food stamp benefits on time.
If you DO NOT return the form, action may be taken to close your case. This action may include your cash assistance, food stamps and/or Medicaid (55 Pa Code 133.84(d), 104.401, 140.513(3), 201.1, 201.3 and 7 CFR 273.12 (a)(1)(viii)).
.If you disagree with the decision to reduce or stop your benefit(s), you have the right to appeal. You will be sent a notice to tell you about any proposed reduction or stoppage of your benefits.
If your case is closed, you may have to complete a new application and be otherwise eligible to have benefits restored.
GOOD CAUSE
YOU MAY CLAIM "GOOD CAUSE" if you have good reason for not completing the form or for returning it late. To claim "good cause", you must state your reason(s) in the space below, sign your statement and return this form to the county assistance office as soon as possible, within 30 days from the due date. You may also claim "good cause" orally by contacting your caseworker, but you must also return this form to the county assistance office as soon as possible, within 30 days from the due date.
I AM CLAIMING "GOOD CAUSE" BECAUSE:
CLIENT SIGNATURE:
For DPW use ONLY
-PAGE A-
|
|
Page 7 |
COMMONWEALTH OF PENNSYLVANIA |
DEPARTMENT OF PUBLIC WELFARE |
PA564 |