
patient summary form pdf can be filled out without difficulty. Simply use FormsPal PDF editor to get it done promptly. Our professional team is constantly working to develop the editor and make it much faster for people with its handy features. Bring your experience one stage further with constantly improving and interesting opportunities we provide! Here is what you'll need to do to start:
Step 1: Just click the "Get Form Button" in the top section of this webpage to see our pdf form editing tool. This way, you'll find everything that is necessary to work with your document.
Step 2: Once you access the PDF editor, there'll be the document made ready to be filled out. Besides filling in various blank fields, you may also perform several other things with the file, including adding any textual content, editing the original textual content, adding illustrations or photos, putting your signature on the form, and more.
As for the blanks of this precise PDF, here's what you should consider:
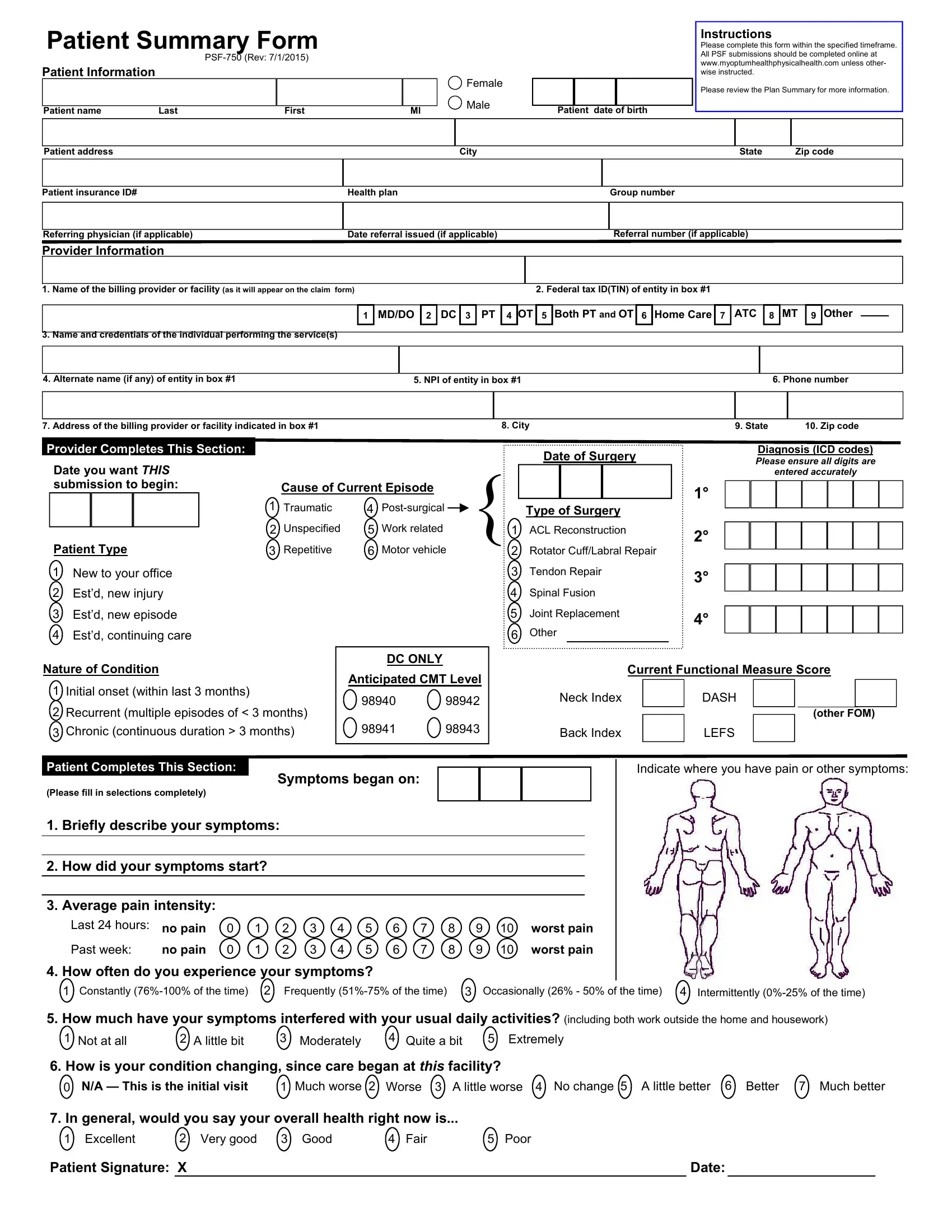
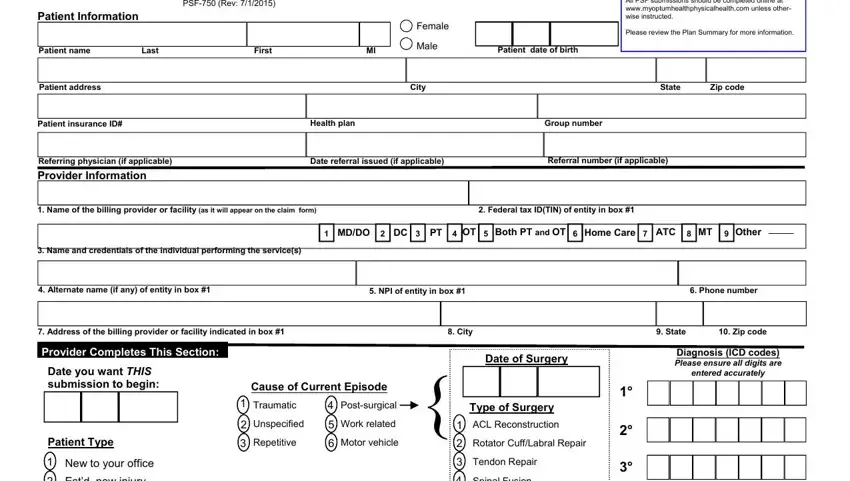
1. Fill out your patient summary form pdf with a group of necessary fields. Collect all of the important information and be sure not a single thing neglected!
2. The next part is to complete the following blank fields: New to your office Estd new injury, Nature of Condition, Spinal Fusion, Joint Replacement, Other, Initial onset within last months, Recurrent multiple episodes of, Chronic continuous duration, Back Index, LEFS, DC ONLY, Anticipated CMT Level, Current Functional Measure Score, Neck Index, and DASH.
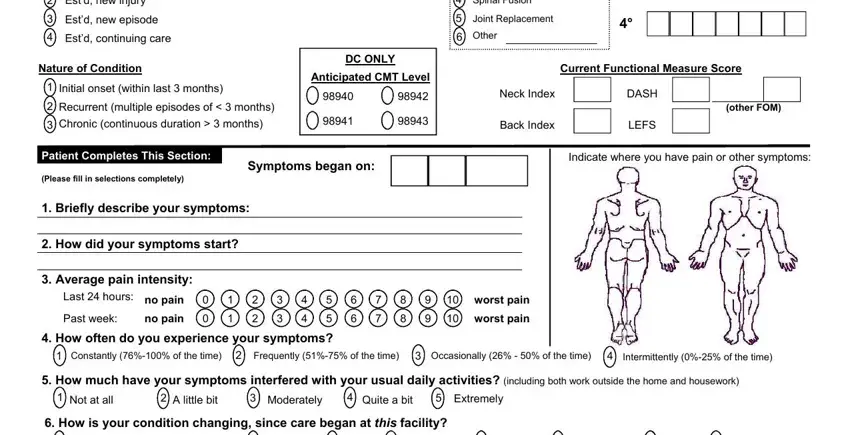
3. The next segment is considered quite easy, NA This is the initial visit, Much worse, Worse, A little worse, No change, A little better, Better, Much better, In general would you say your, Excellent, Very good, Good, Fair, Poor, and Patient Signature X - all these empty fields must be filled out here.

People generally make mistakes when filling in Patient Signature X in this part. You should definitely read twice whatever you enter here.
Step 3: Soon after rereading your fields you have filled in, press "Done" and you're good to go! Right after starting afree trial account here, you will be able to download patient summary form pdf or send it via email immediately. The file will also be available through your personal cabinet with your each change. If you use FormsPal, you're able to complete forms without the need to get worried about data incidents or entries being shared. Our protected software makes sure that your private data is maintained safely.