
In case you want to fill out Orthodontia, you don't have to download any sort of software - just try using our PDF tool. In order to make our tool better and easier to use, we constantly work on new features, considering suggestions coming from our users. To get started on your journey, consider these simple steps:
Step 1: Access the PDF form inside our tool by clicking on the "Get Form Button" above on this page.
Step 2: The editor helps you customize PDF files in a variety of ways. Modify it by writing your own text, adjust existing content, and add a signature - all within the reach of several mouse clicks!
This document will require specific details to be filled in, hence make sure you take whatever time to fill in precisely what is asked:
1. It is very important complete the Orthodontia accurately, therefore be attentive while filling in the parts comprising all of these fields:
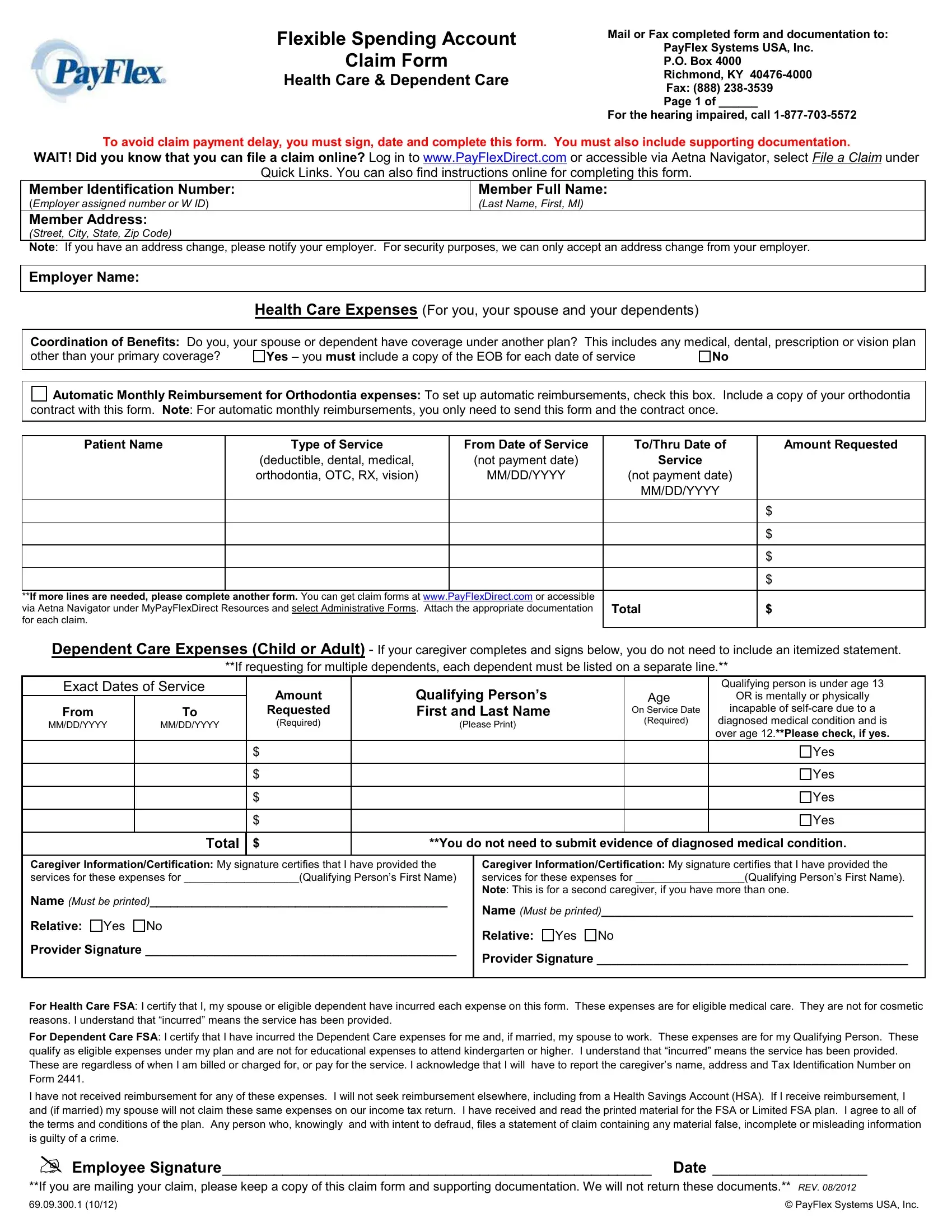
2. Right after completing the previous step, head on to the subsequent step and fill out the essential particulars in these blanks - If more lines are needed please, Total, Dependent Care Expenses Child or, If requesting for multiple, Exact Dates of Service, From, MMDDYYYY, MMDDYYYY, Amount, Requested, Required, Qualifying Persons First and Last, Please Print, Age On Service Date, and Required.
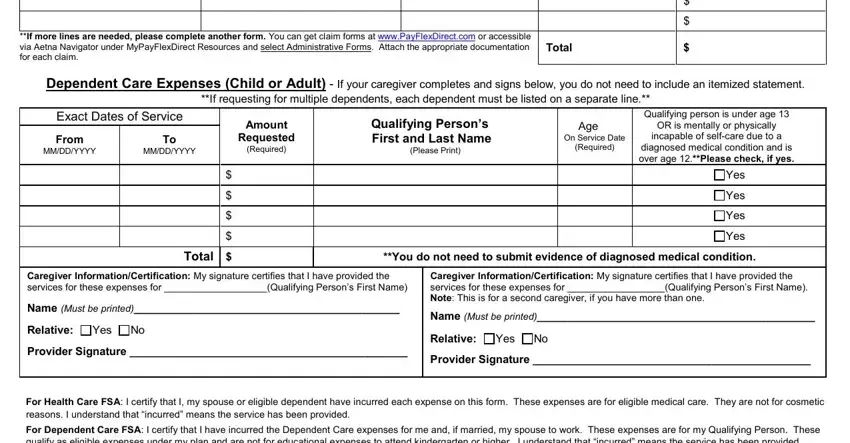
3. The following section focuses on I have not received reimbursement, Employee Signature Date, If you are mailing your claim, and PayFlex Systems USA Inc - fill in all of these fields.

As for PayFlex Systems USA Inc and If you are mailing your claim, be sure you get them right in this current part. Both of these are the most important ones in this document.
Step 3: Check all the details you've entered into the form fields and then hit the "Done" button. Right after setting up afree trial account with us, it will be possible to download Orthodontia or email it immediately. The PDF file will also be accessible via your personal account menu with all your edits. FormsPal is committed to the confidentiality of our users; we make sure that all personal data handled by our system is protected.