MEDICAL RECORD-SUPPLEMENTAL MEDICAL DATA
For use of this form, see AR 40-66; the proponent agency is the Office of The Surgeon General
REPORT TITLE Physical Therapy Medical History Intake Form Neck Pain
|
MOS/Occupation: |
|
|
|
|
|
|
|
|
|
|
|
Medical History: |
|
Self |
│ |
Family |
|
Duty Station/Unit: |
|
|
|
|
|
|
|
|
|
|
|
Cancer? |
Yes |
No |
│ |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
Diabetes? |
Yes |
No |
│ |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
When did symptoms start (date): |
|
|
|
|
|
|
|
|
High Blood Pressure? |
Yes |
No |
│ |
Yes |
No |
|
Symptoms related to deployment? □Yes-Combat □Yes-NonCombat □No |
Heart Disease? |
Yes |
No |
│ |
Yes |
No |
|
Osteoporosis? |
Yes |
No |
│ |
Yes |
No |
|
Have you had these symptoms before? □Yes |
□No |
|
|
|
|
Osteoarthritis? |
Yes |
No |
│ |
Yes |
No |
|
How did symptoms start? |
|
|
|
|
|
|
|
|
|
|
Rheumatoid arthritis? |
Yes |
No |
│ |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
Neurologic dz (MS, Parkinsons)? |
Yes |
No |
│ |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
Symptoms are? |
□Constant |
|
□Come/Go |
|
□Only with Activity |
Ulcers / GERD / Acid Reflux? |
Yes |
No |
│ |
Yes |
No |
|
Symptoms are? |
□Getting worse |
□Not Changing |
□Getting Better |
Kidney / Liver Disease? |
Yes |
No |
│ |
Yes |
No |
|
Prior Surgeries: |
Yes |
No |
│ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
List any medications or dietary supplements your are taking: |
|
|
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In the past 3 months have you had or do you experience: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
□None |
Change in your general health? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fever / chills / sweats? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
List any drug or latex allergies you are aware of: |
|
|
|
□None |
Unexplained weight change (>10lbs)? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Numbness or tingling? |
|
Yes |
No |
|
|
List Assistive Devices you use (crutches, braces, shoe inserts): |
|
|
Bowel / bladder incontinence? |
|
Yes |
No |
|
|
□None |
Difficulty sleeping due to pain? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unexplained Falls/Decreased balance? |
Yes |
No |
|
|
Are you in the Personal Reliability Program (PRP)? |
□Yes |
□No |
|
|
Are you currently/Do you have: |
|
|
|
|
|
|
Have you completed advanced medical directives? |
□Yes |
□No |
Pregnant / Potentially Pregnant / Nursing? |
|
NA |
Yes |
No |
|
Often bothered by feeling down, depressed, or hopeless? |
Yes |
No |
|
(aka: “living will”) |
Information is available at front desk. |
|
|
|
|
|
|
|
Often bothered by little interest or pleasure in doing things? Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Do you have difficulties with? (check all that apply) |
|
|
|
|
Under physical / emotional abuse? |
|
|
|
Yes |
No |
|
□Communication |
□Vision |
|
|
□None |
|
|
|
|
|
Dietary or Nutritional Concerns? |
|
|
|
Yes |
No |
|
□Speech |
|
|
□Hearing |
|
|
□Other: |
|
|
|
|
|
|
Do you use tobacco products? |
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
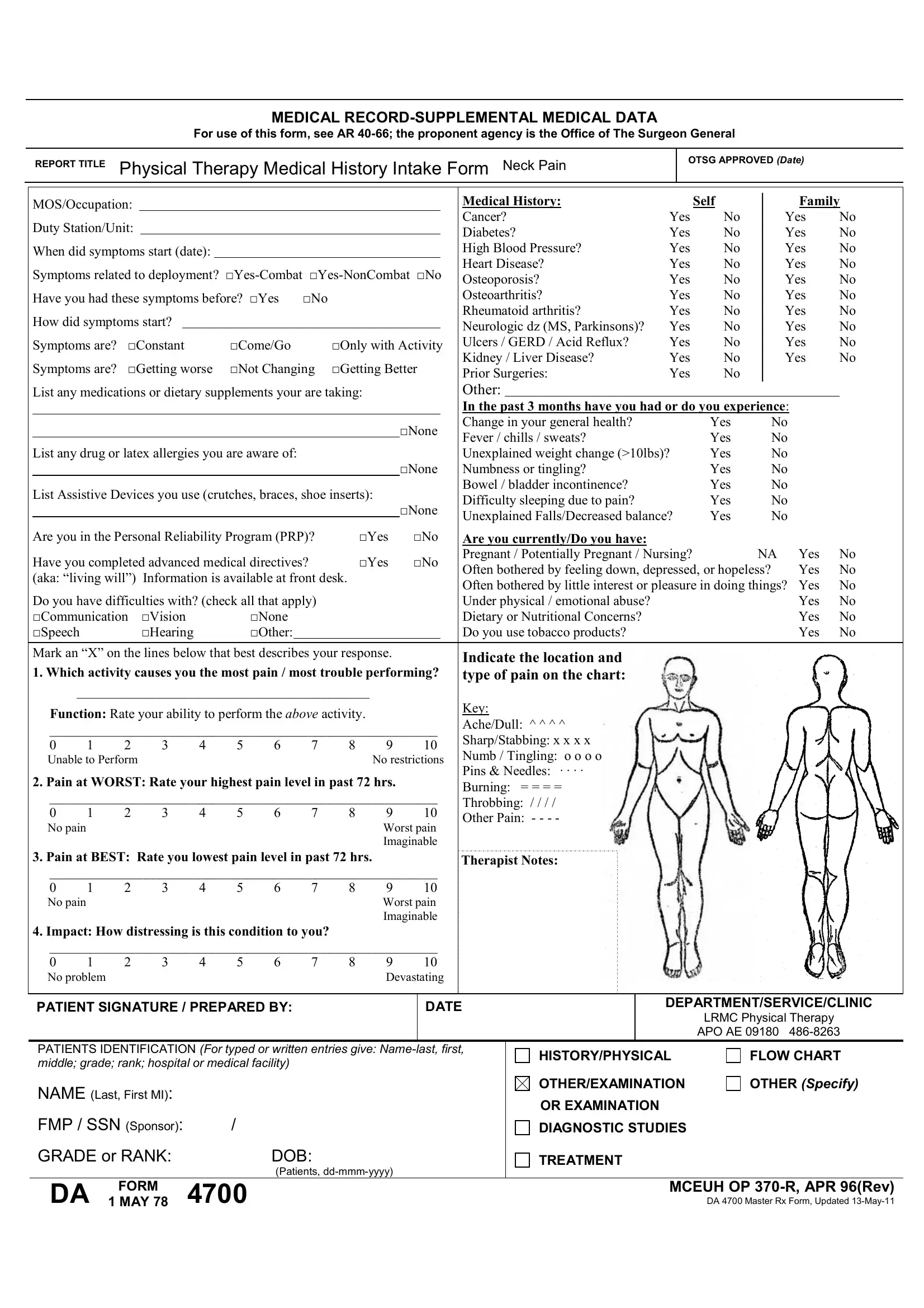
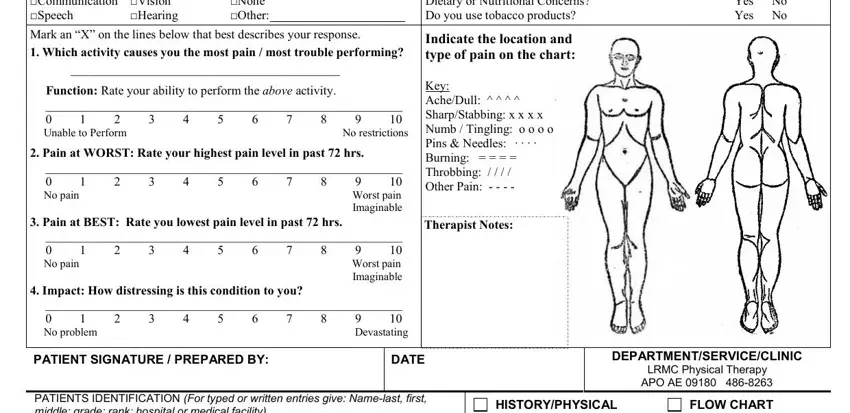
Mark an “X” on the lines below that best describes your response. |
|
|
Indicate the location and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. Which activity causes you the most pain / most trouble performing? |
type of pain on the chart: |
|
|
|
|
|
|
___________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
Function: Rate your ability to perform the ABOVE activity. |
|
|
|
Key: |
|
|
|
|
|
|
|
|
|
Ache/Dull: ^ ^ ^ ^ |
|
|
|
|
|
|
_________________________________________________________ |
|
|
|
|
|
|
|
|
Sharp/Stabbing: x x x x |
|
|
|
|
|
|
0 |
1 |
2 |
3 |
|
4 |
5 |
6 |
|
7 |
8 |
9 |
10 |
|
|
|
|
|
|
|
|
|
|
Numb / Tingling: o o o o |
|
|
|
|
|
|
Unable to Perform |
|
|
|
|
|
|
|
|
No restrictions |
|
|
|
|
|
|
2. Pain at WORST: Rate your highest pain level in past 72 hrs. |
|
|
Pins & Needles: · · · · |
|
|
|
|
|
|
|
|
Burning: = = = = |
|
|
|
|
|
|
_________________________________________________________ |
|
|
|
|
|
|
|
|
Throbbing: / / / / |
|
|
|
|
|
|
0 |
1 |
2 |
3 |
|
4 |
5 |
6 |
|
7 |
8 |
9 |
10 |
|
|
|
|
|
|
|
|
|
|
Other Pain: - - - - |
|
|
|
|
|
|
No pain |
|
|
|
|
|
|
|
|
|
|
Worst pain |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Imaginable |
|
|
|
|
|
|
|
|
3. Pain at BEST: Rate you lowest pain level in past 72 hrs. |
|
|
|
Therapist Notes: |
|
|
|
|
|
|
_________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
1 |
2 |
3 |
|
4 |
5 |
6 |
|
7 |
8 |
9 |
10 |
|
|
|
|
|
|
|
|
|
No pain |
|
|
|
|
|
|
|
|
|
|
Worst pain |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Imaginable |
|
|
|
|
|
|
|
4.Impact: How distressing is this condition to you?
_________________________________________________________
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
No problem |
|
|
|
|
|
|
|
Devastating |
PATIENT SIGNATURE / PREPARED BY:
DEPARTMENT/SERVICE/CLINIC
LRMC Physical Therapy
APO AE 09180 486-8263
PATIENTS IDENTIFICATION (For typed or written entries give: Name-last, first, middle; grade; rank; hospital or medical facility)
NAME (Last, First MI): |
|
FMP / SSN (Sponsor): |
/ |
GRADE or RANK: |
DOB: |
|
(Patients, dd-mmm-yyyy) |
OTHER/EXAMINATION
OR EXAMINATION
DIAGNOSTIC STUDIES
TREATMENT
DA |
FORM |
4700 |
MCEUH OP 370-R, APR 96(Rev) |
1 MAY 78 |
DA 4700 Master Rx Form, Updated 13-May-11 |
NECK DISABILITY INDEX1
Section 1: To be completed by patient |
_______AD |
______Non-Active Duty |
Name:______________________________ |
Age:_______ |
Date:__________________ |
Occupation:_________________________ |
Number of days of neck pain:_____________(this episode) |
|
|
|
Section 2: To be completed by patient |
|
|
This questionnaire has been designed to give your therapist information as to how your neck pain has affected your ability to manage in every day life. Please answer every question by placing a mark on the line that best describes your condition today. We realize you may feel that two of the statements may describe your condition, but please mark only the line which most closely describes your current condition.
Pain Intensity
_____I have no pain at the moment.
_____The pain is very mild at the moment.
_____The pain is moderate at the moment.
_____The pain is fairly severe at the moment.
_____The pain is very severe at the moment.
_____The pain is the worst imaginable at the moment.
Personal Care (Washing, Dressing, etc.)
_____I do not have to change the way I wash and dress myself to avoid pain.
_____I do not normally change the way I wash or dress myself even though it causes some pain.
_____Washing and dressing increases my pain, but I can do it without changing my way of doing it.
_____Washing and dressing increases my pain, and I find it necessary to change the way I do it.
_____Because of my pain I am partially unable to wash and dress without help.
_____Because of my pain I am completely unable to wash or dress without help.
Lifting
_____I can lift heavy weights without increased pain.
_____I can lift heavy weights but it causes increased pain
_____Pain prevents me from lifting heavy weights off of the floor, but I can manage if they are conveniently
positioned (ex. on a table, etc.).
_____Pain prevents me from lifting heavy weights off of the floor, but I can manage light to medium weights
if they are conveniently positioned.
_____I can lift only very light weights.
_____I can not lift or carry anything at all.
Reading
_____I can read as much as I want to with no pain in my neck.
_____I can read as much as I want to with slight pain in my neck.
_____I can read as much as I want with moderate pain in my neck.
_____I can’t read as much as I want because of moderate pain in my neck.
_____I can hardly read at all because of severe pain in my neck.
_____I cannot read at all.
Headache
_____I have no headache at all.
_____I have slight headaches which come infrequently.
_____I have moderate headaches which come infrequently.
_____I have moderate headaches which come frequently.
_____I have severe headaches which come frequently.
_____I have headaches almost all the time.
(Don’t forget to fill out the back side)
NECK DISABILITY INDEX, p. 2
Section 2 (con’t): To be completed by patient
Concentration
_____I can concentrate fully when I want to with no difficulty.
_____I can concentrate fully when I want to with slight difficulty.
_____I have a fair degree of difficulty in concentrating when I want to.
_____I have a lot of difficulty in concentrating when I want to.
_____I have a great deal of difficulty in concentrating when I want to.
_____I cannot concentrate at all.
Work
_____I can do as much as I want to.
_____I can only do my usual work but no more.
_____I can do most of my usual work, but no more.
_____I cannot do my usual work.
_____I can hardly do any work at all.
_____I can’t do any work at all.
Driving
_____I can drive my car without any neck pain.
_____I can drive my car as long as I want with slight pain in my neck.
_____I can drive my car as long as I want with moderate pain in my neck.
_____I can’t drive my car as long as I want because of moderate pain in my neck.
_____I can hardly drive at all because of severe pain in my neck.
_____I can’t drive my car at all.
Sleeping
_____I have no trouble sleeping.
_____My sleep is slightly disturbed (less than 1 hour sleep loss).
_____My sleep is mildly disturbed (1-2 hour sleep loss).
_____My sleep is moderately disturbed (2-3 hours sleep loss).
_____My sleep is greatly disturbed (3-5 hours sleep loss).
_____My sleep is completely disturbed (5-7 hours sleep loss).
Recreation
_____I am able to engage in all my recreational activities with no neck pain at all.
_____I am able to engage in all my recreational activities with some pain in my neck.
_____I am able to engage in most but not all of my usual recreational activities because of pain in my neck.
_____I am able to engage in a few of my usual recreational activities because of pain in my neck.
_____I can hardly do any recreational activities because of pain in my neck.
____ I can’t do any recreational activities at all.
Section 3: To be completed by physical therapist/provider |
|
|
|
|
SCORE:________out of 50 (SEM 5, MDC 7) |
Initial |
F/U ___ weeks |
Discharge |
Number of treatment sessions:________________ |
Gender: |
Male |
Female |
Diagnosis/ICD-9 Code:_______________________ |
|
|
|
|
1Adapted from Vernon H, Mior S. The Neck Disability Indes: A Study of Reliability and Validitiy. Journal of Manipulative and Physiological Therapeutics 1991; 14(7): 409-415.