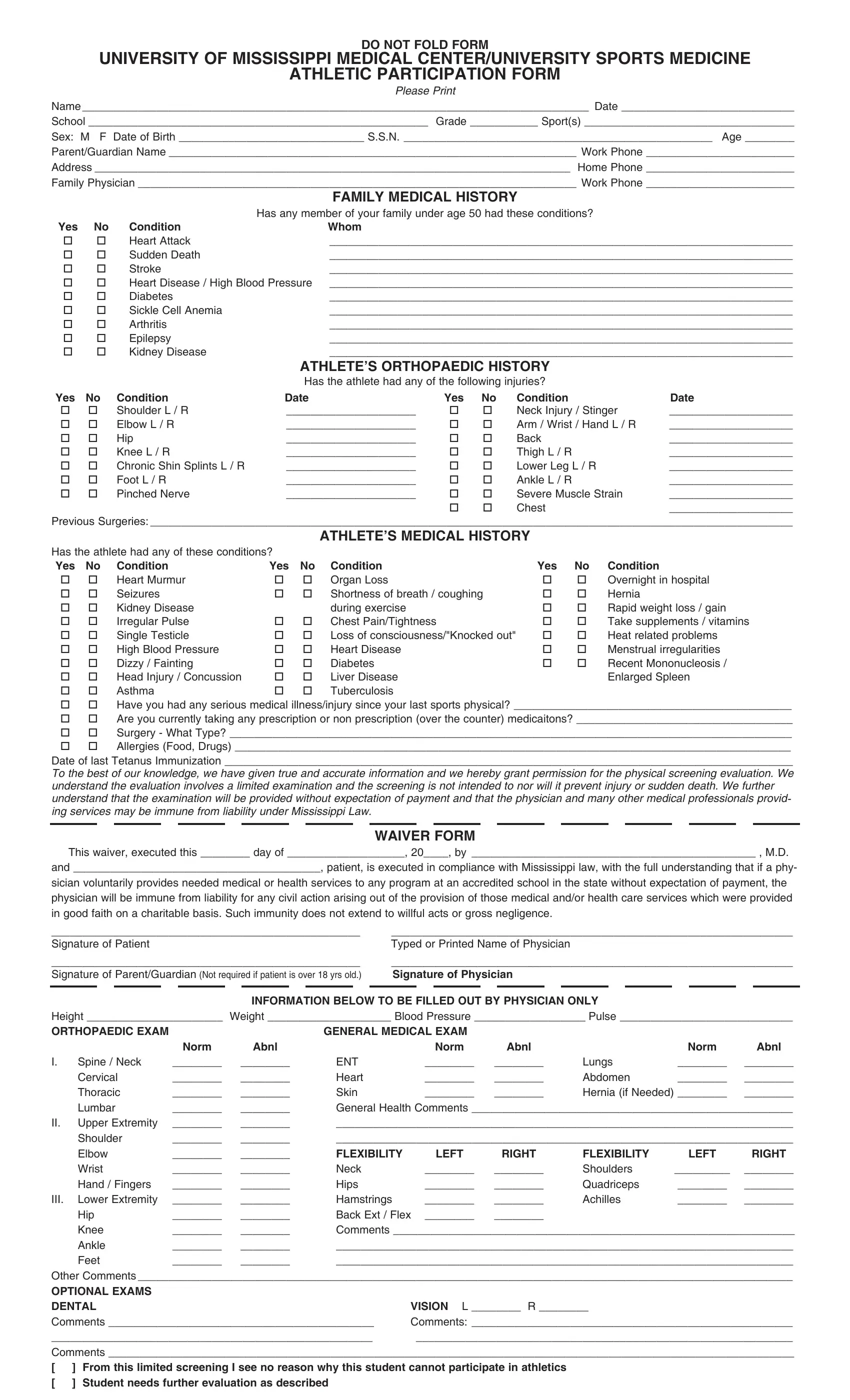
DO NOT FOLD FORM
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER/UNIVERSITY SPORTS MEDICINE
ATHLETIC PARTICIPATION FORM
Please Print
Name __________________________________________________________________________________ Date ____________________________
School _______________________________________________________ Grade ___________ Sport(s) __________________________________
Sex: M F Date of Birth ______________________________ S.S.N. __________________________________________________ Age ________
Parent/Guardian Name __________________________________________________________________ Work Phone ________________________
Address _____________________________________________________________________________ Home Phone ________________________
Family Physician _______________________________________________________________________ Work Phone ________________________
|
|
|
FAMILY MEDICAL HISTORY |
|
|
|
|
Has any member of your family under age 50 had these conditions? |
|
Yes |
No |
Condition |
Whom |
|
|
|
|
|
|
Heart Attack |
___________________________________________________________________________ |
|
|
Sudden Death |
___________________________________________________________________________ |
|
|
Stroke |
___________________________________________________________________________ |
|
|
Heart Disease / High Blood Pressure ___________________________________________________________________________ |
|
|
Diabetes |
___________________________________________________________________________ |
|
|
Sickle Cell Anemia |
___________________________________________________________________________ |
|
|
Arthritis |
___________________________________________________________________________ |
|
|
Epilepsy |
___________________________________________________________________________ |
|
|
Kidney Disease |
___________________________________________________________________________ |
|
|
|
ATHLETE’S ORTHOPAEDIC HISTORY |
|
|
|
|
Has the athlete had any of the following injuries? |
|
Yes |
No |
Condition |
Date |
Yes |
No |
Condition |
Date |
|
|
Shoulder L / R |
_____________________ |
|
|
Neck Injury / Stinger |
____________________ |
|
|
Elbow L / R |
_____________________ |
|
|
Arm / Wrist / Hand L / R |
____________________ |
|
|
Hip |
_____________________ |
|
|
Back |
____________________ |
|
|
Knee L / R |
_____________________ |
|
|
Thigh L / R |
____________________ |
|
|
Chronic Shin Splints L / R |
_____________________ |
|
|
Lower Leg L / R |
____________________ |
|
|
Foot L / R |
_____________________ |
|
|
Ankle L / R |
____________________ |
|
|
Pinched Nerve |
_____________________ |
|
|
Severe Muscle Strain |
____________________ |
|
|
|
|
|
|
Chest |
____________________ |
Previous Surgeries: ________________________________________________________________________________________________________
ATHLETE’S MEDICAL HISTORY
Has the athlete had any of these conditions? |
|
|
|
|
|
Yes |
No |
Condition |
Yes |
No |
Condition |
Yes |
No |
Condition |
|
|
Heart Murmur |
|
|
Organ Loss |
|
|
Overnight in hospital |
|
|
Seizures |
|
|
Shortness of breath / coughing |
|
|
Hernia |
|
|
Kidney Disease |
|
|
during exercise |
|
|
Rapid weight loss / gain |
|
|
Irregular Pulse |
|
|
Chest Pain/Tightness |
|
|
Take supplements / vitamins |
|
|
Single Testicle |
|
|
Loss of consciousness/"Knocked out" |
|
|
Heat related problems |
|
|
High Blood Pressure |
|
|
Heart Disease |
|
|
Menstrual irregularities |
|
|
Dizzy / Fainting |
|
|
Diabetes |
|
|
Recent Mononucleosis / |
|
|
Head Injury / Concussion |
|
|
Liver Disease |
|
|
Enlarged Spleen |
|
|
Asthma |
|
|
Tuberculosis |
|
|
|
Have you had any serious medical illness/injury since your last sports physical? _____________________________________________
Are you currently taking any prescription or non prescription (over the counter) medicaitons? ___________________________________
Surgery - What Type? ___________________________________________________________________________________________
Allergies (Food, Drugs) __________________________________________________________________________________________
Date of last Tetanus Immunization ____________________________________________________________________________________________
To the best of our knowledge, we have given true and accurate information and we hereby grant permission for the physical screening evaluation. We understand the evaluation involves a limited examination and the screening is not intended to nor will it prevent injury or sudden death. We further understand that the examination will be provided without expectation of payment and that the physician and many other medical professionals provid- ing services may be immune from liability under Mississippi Law.
WAIVER FORM
This waiver, executed this ________ day of ___________________, 20____, by ______________________________________________ , M.D.
and ________________________________________, patient, is executed in compliance with Mississippi law, with the full understanding that if a phy-
sician voluntarily provides needed medical or health services to any program at an accredited school in the state without expectation of payment, the physician will be immune from liability for any civil action arising out of the provision of those medical and/or health care services which were provided in good faith on a charitable basis. Such immunity does not extend to willful acts or gross negligence.
__________________________________________________ |
_________________________________________________________________ |
Signature of Patient |
|
|
|
Typed or Printed Name of Physician |
|
|
|
__________________________________________________ |
_________________________________________________________________ |
Signature of Parent/Guardian (Not required if patient is over 18 yrs old.) |
Signature of Physician |
|
|
|
|
|
|
INFORMATION BELOW TO BE FILLED OUT BY PHYSICIAN ONLY |
|
|
Height ______________________ |
Weight ____________________ Blood Pressure __________________ Pulse ____________________________ |
ORTHOPAEDIC EXAM |
|
|
GENERAL MEDICAL EXAM |
|
|
|
|
|
|
Norm |
Abnl |
|
|
Norm |
Abnl |
|
Norm |
Abnl |
I. |
Spine / Neck |
________ |
________ |
ENT |
|
________ |
________ |
Lungs |
________ |
________ |
|
Cervical |
________ |
________ |
Heart |
|
________ |
________ |
Abdomen |
________ |
________ |
|
Thoracic |
________ |
________ |
Skin |
|
________ |
________ |
Hernia (if Needed) ________ |
________ |
|
Lumbar |
________ |
________ |
General Health Comments ____________________________________________________ |
II. |
Upper Extremity |
________ |
________ |
__________________________________________________________________________ |
|
Shoulder |
________ |
________ |
__________________________________________________________________________ |
|
Elbow |
________ |
________ |
FLEXIBILITY |
LEFT |
RIGHT |
FLEXIBILITY |
LEFT |
RIGHT |
|
Wrist |
________ |
________ |
Neck |
|
________ |
________ |
Shoulders |
_________ |
________ |
|
Hand / Fingers |
________ |
________ |
Hips |
|
________ |
________ |
Quadriceps |
________ |
________ |
III. |
Lower Extremity |
________ |
________ |
Hamstrings |
________ |
________ |
Achilles |
________ |
________ |
|
Hip |
________ |
________ |
Back Ext / Flex |
________ |
________ |
|
|
|
|
Knee |
________ |
________ |
Comments _________________________________________________________________ |
|
Ankle |
________ |
________ |
__________________________________________________________________________ |
|
Feet |
________ |
________ |
__________________________________________________________________________ |
Other Comments __________________________________________________________________________________________________________
OPTIONAL EXAMS |
|
DENTAL |
VISION L ________ R ________ |
Comments ___________________________________________ |
Comments: ____________________________________________________ |
____________________________________________________ |
_____________________________________________________________ |
Comments _______________________________________________________________________________________________________________
[ |
] |
From this limited screening I see no reason why this student cannot participate in athletics |
[ |
] |
Student needs further evaluation as described |