The PDF editor that you're going to begin using was developed by our main computer programmers. One could get the pod form 265 form immediately and without problems using this application. Just keep up with this particular guideline to start out.
Step 1: Select the button "Get Form Here".
Step 2: So you are going to be on the file edit page. It's possible to add, adjust, highlight, check, cross, insert or delete fields or phrases.
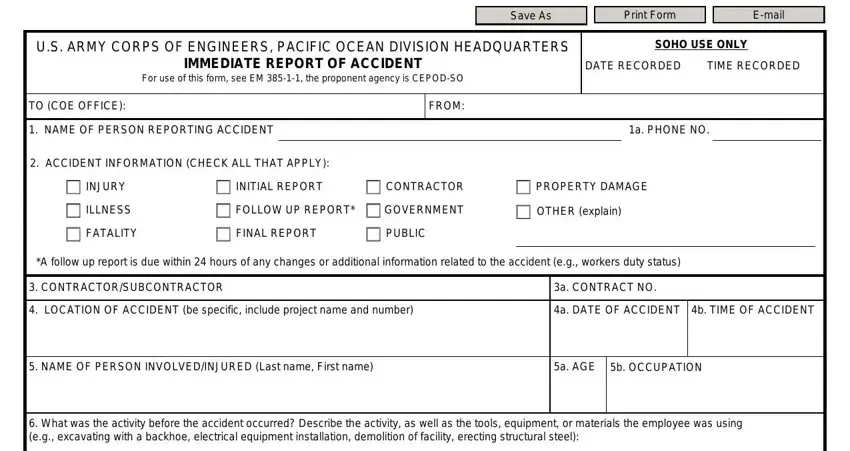
Make sure you provide the following information to fill out the pod form 265 PDF:
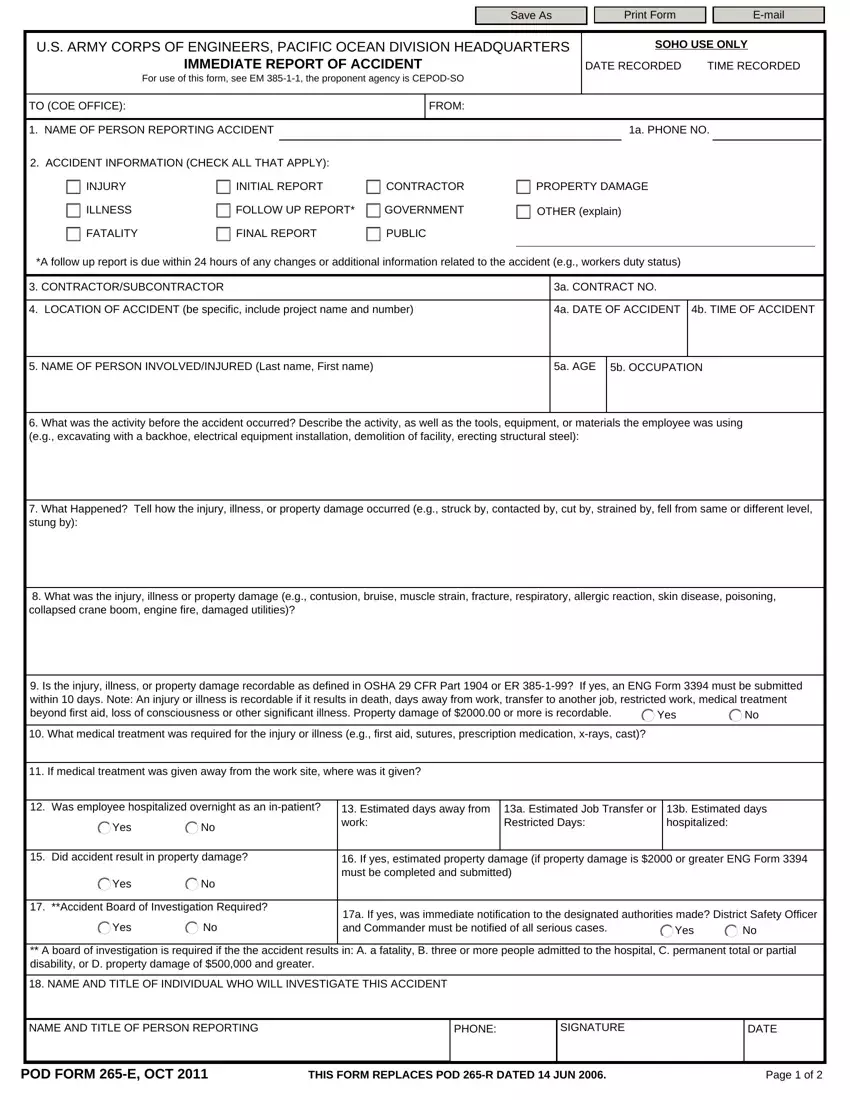
Fill in the What Happened Tell how the injury, What was the injury illness or, Is the injury illness or property, Yes, What medical treatment was, If medical treatment was given, Was employee hospitalized, Yes, Estimated days away from work, a Estimated Job Transfer or, b Estimated days hospitalized, Did accident result in property, Yes, Accident Board of Investigation, and If yes estimated property damage section with the details asked by the application.
Record any particulars you need within the field Yes, a If yes was immediate, Yes, A board of investigation is, NAME AND TITLE OF INDIVIDUAL WHO, NAME AND TITLE OF PERSON REPORTING, PHONE, SIGNATURE, DATE, POD FORM E OCT, THIS FORM REPLACES POD R DATED, and Page of.
When it comes to paragraph CONTINUATION PAGE, identify the rights and obligations.
Step 3: Choose the "Done" button. You can now transfer your PDF document to your electronic device. As well as that, you may forward it by means of email.
Step 4: To prevent possible upcoming troubles, ensure that you have up to several copies of every single file.
