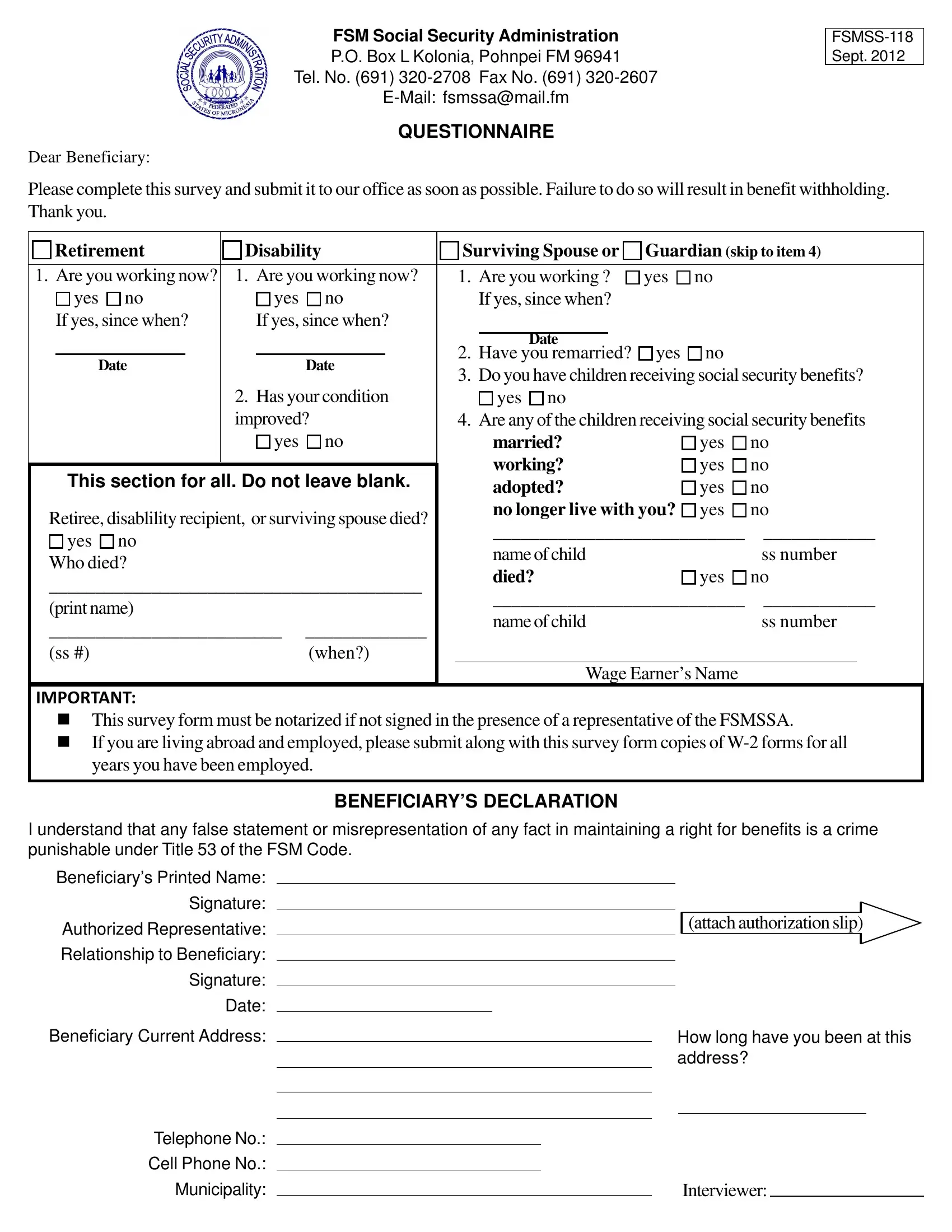
In addressing the complexities of navigating social security benefits within the Federated States of Micronesia, particularly in Pohnpei, the Pohnpei Social Security form serves as a critical tool for beneficiaries to maintain their eligibility and ensure the proper administration of their benefits. Issued by the FSM Social Security Administration, this form, FSMSS-118, as of September 2012, acts as a comprehensive questionnaire tailored towards retirees, individuals with disabilities, and surviving spouses or guardians. By requiring detailed information about employment status, marital changes, and the status of children who may also receive benefits, it emphasizes the administration's efforts to accurately assess benefit eligibility and need. Particularly noteworthy is the form's requirements for notarization or its equivalent authentication when the beneficiary is unable to sign in the presence of an FSMSSA representative, underscoring the importance of legal accuracy and accountability in the process. Included are directives for those living abroad, indicating the necessity of W-2 forms submission for employed beneficiaries, highlighting the global considerations the administration accommodates. Moreover, the declaration section at the form's conclusion, warning against false statements under penalty of law, reflects the legal gravitas and ethical seriousness with which this process is imbued. Overall, the Pohnpei Social Security form encompasses a vital, legally grounded, and ethically significant step for beneficiaries within the FSM Social Security system, ensuring that aid is appropriately and justly distributed.
| Question | Answer |
|---|---|
| Form Name | Pohnpei Social Security Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | social security administration baltimore, fsmss118, fsmss118 pdf, social security benefits print out |
FSM Social Security Administration
P.O. Box L Kolonia, Pohnpei FM 96941
Tel. No. (691)
QUESTIONNAIRE
Dear Beneficiary:
Please complete this survey and submit it to our office as soon as possible. Failure to do so will result in benefit withholding. Thank you.
Retirement |
Disability |
|
Surviving Spouse or |
Guardian (skip to item 4) |
||||||||||||
|
|
|
|
|
|
|
|
|||||||||
1. Are you working now? |
1. Are you working now? |
|
1. Are you working ? |
yes |
no |
|
|
|||||||||
|
yes |
no |
|
yes |
no |
|
|
If yes, since when? |
|
|
|
|
||||
If yes, since when? |
|
If yes, since when? |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Have you remarried? |
yes |
no |
|
|
|||
|
Date |
|
|
Date |
|
|
||||||||||
|
|
|
|
3. Do you have children receiving social security benefits? |
||||||||||||
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
2. Has your condition |
|
|
yes no |
|
|
|
|
|||||
|
|
|
|
improved? |
|
4. Are any of the children receiving social security benefits |
||||||||||
|
|
|
|
|
yes |
no |
|
|
married? |
|
yes |
no |
||||
|
|
|
|
|
|
|
|
|
|
working? |
|
yes |
no |
|||
|
This section for all. Do not leave blank. |
|
|
|
||||||||||||
|
|
|
adopted? |
|
yes |
no |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
Retiree, disablility recipient, or surviving spouse died? |
|
|
no longer live with you? |
yes |
no |
|||||||||||
___________________________ |
____________ |
|||||||||||||||
|
yes |
no |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
name of child |
|
|
ss number |
||||||
Who died? |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
died? |
|
yes |
no |
|||||||
________________________________________ |
|
|
|
|||||||||||||
___________________________ |
____________ |
|||||||||||||||
(print name) |
|
|
|
|
||||||||||||
|
|
|
|
|
|
name of child |
|
|
ss number |
|||||||
_________________________ |
_____________ |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|||||||||
(ss #) |
|
|
|
|
(when?) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Wage Earner’s Name |
|
|
||||
IMPORTANT:
nThis survey form must be notarized if not signed in the presence of a representative of the FSMSSA.
nIf you are living abroad and employed, please submit along with this survey form copies of
BENEFICIARY’S DECLARATION
I understand that any false statement or misrepresentation of any fact in maintaining a right for benefits is a crime punishable under Title 53 of the FSM Code.
Beneficiary’s Printed Name:
Signature:
Authorized Representative:
Relationship to Beneficiary:
Signature:
Date:
Beneficiary Current Address:
Telephone No.:
Cell Phone No.:
Municipality:
(attach authorization slip)
How long have you been at this address?
Interviewer: