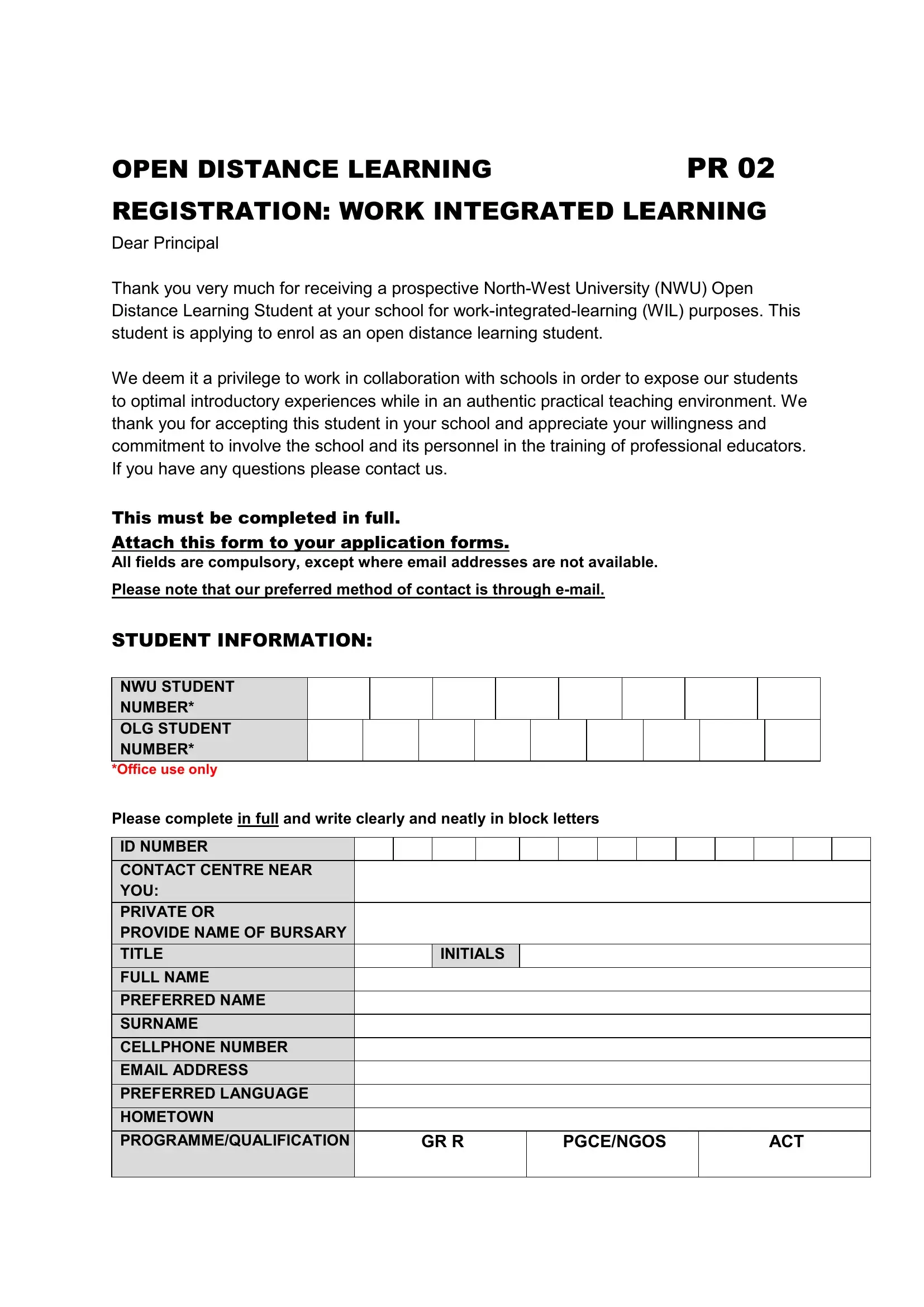
The PR 02 form signifies a critical step for students embarking on a journey through the Open Distance Learning (ODL) at North-West University (NWU). It serves as the bridge connecting prospective students with schools for Work-Integrated Learning (WIL), a cornerstone for hands-on experience in the teaching field. Each section meticulously collects information from students and the participating schools, ensuring a seamless integration into practical teaching environments. The form delineates clear instructions for completion, emphasizing the necessity of detailed information like student identification, contact details, program of study, and current employment status. Schools play a pivotal role in this process, providing essential data such as grade offerings, language mediums, and mentorship details. Of particular importance is the signature of both the student and the principal, symbolizing a mutual commitment to the educational journey ahead. Moreover, the form highlights the importance of communication, predominantly via email, to facilitate efficient interactions among all parties involved. Through this form, NWU strengthens its partnerships with schools, fostering professional educator training grounded in real-world experience.
| Question | Answer |
|---|---|
| Form Name | Pr 02 Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | pr02, what is a pr02 form, pr 02 form, pr02 forms |
