The proof of pregnancy form from doctor completing process is very simple. Our editor lets you work with any PDF document.
Step 1: The initial step should be to click on the orange "Get Form Now" button.
Step 2: At the time you access our proof of pregnancy form from doctor editing page, you will find all the actions you can take regarding your template at the upper menu.
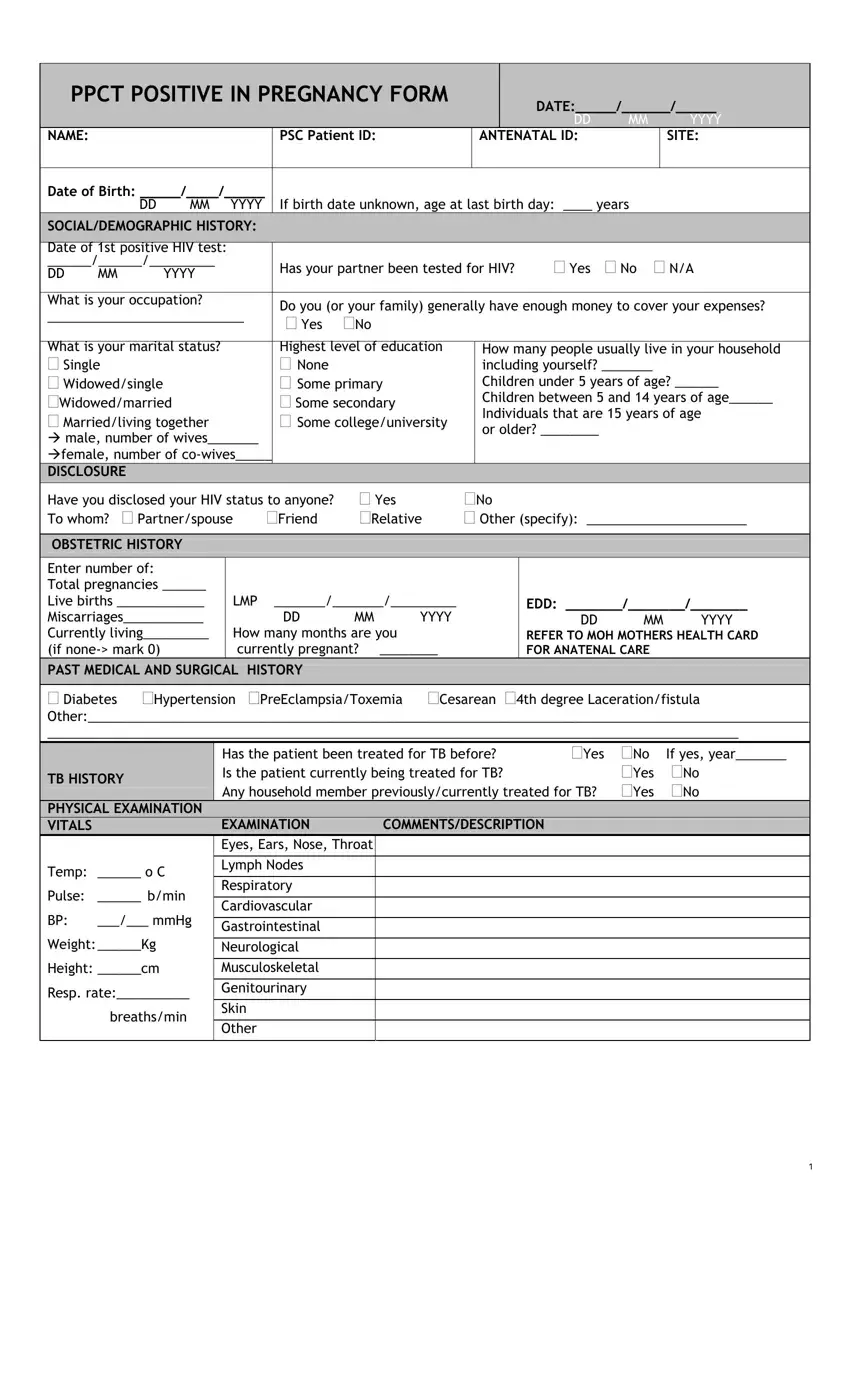
These sections will make up your PDF form:
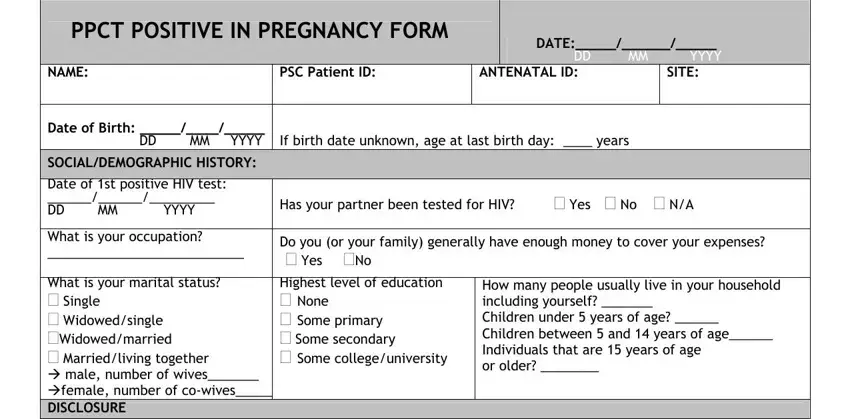
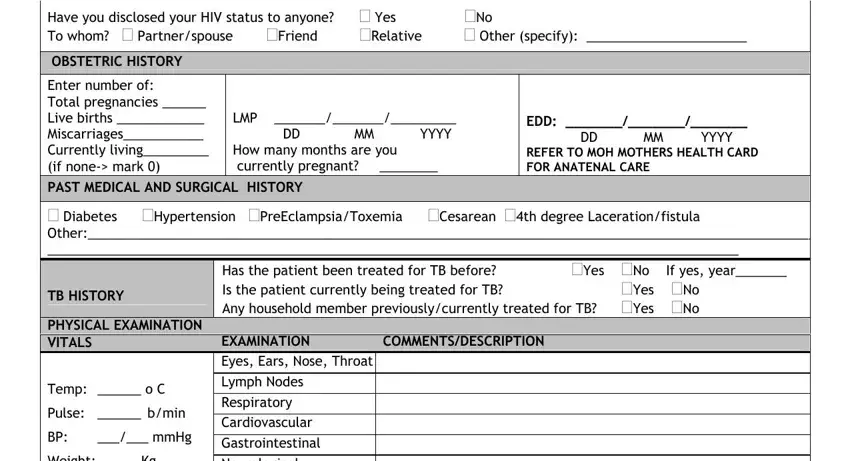
Type in the necessary details in the area Have you disclosed your HIV status, OBSTETRIC HISTORY, Enter number of Total pregnancies, LMP DD MM YYYY How many months, EDD DD MM YYYY REFER TO MOH, Diabetes Hypertension, TB HISTORY, PHYSICAL EXAMINATION VITALS, Temp o C, Pulse bmin, mmHg, Weight Kg, Has the patient been treated for, COMMENTSDESCRIPTION, and EXAMINATION Eyes Ears Nose Throat.
Provide the necessary details in the Weight Kg, Height cm, Resp rate, breathsmin, and EXAMINATION Eyes Ears Nose Throat field.
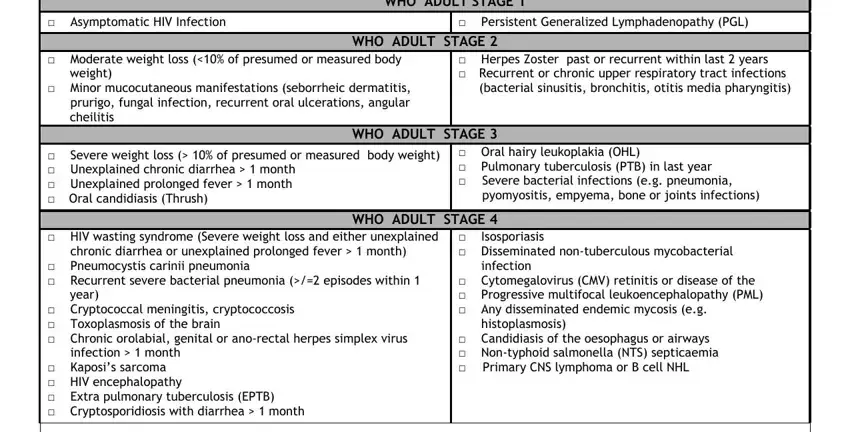
You have to define the rights and obligations of all parties in box WHO ADULT STAGE, Asymptomatic HIV Infection, Persistent Generalized, WHO ADULT STAGE, Moderate weight loss of presumed, cheilitis, Herpes Zoster past or recurrent, bacterial sinusitis bronchitis, WHO ADULT STAGE, Severe weight loss of presumed, Oral hairy leukoplakia OHL, Severe bacterial infections eg, HIV wasting syndrome Severe, Isosporiasis, and Disseminated nontuberculous.
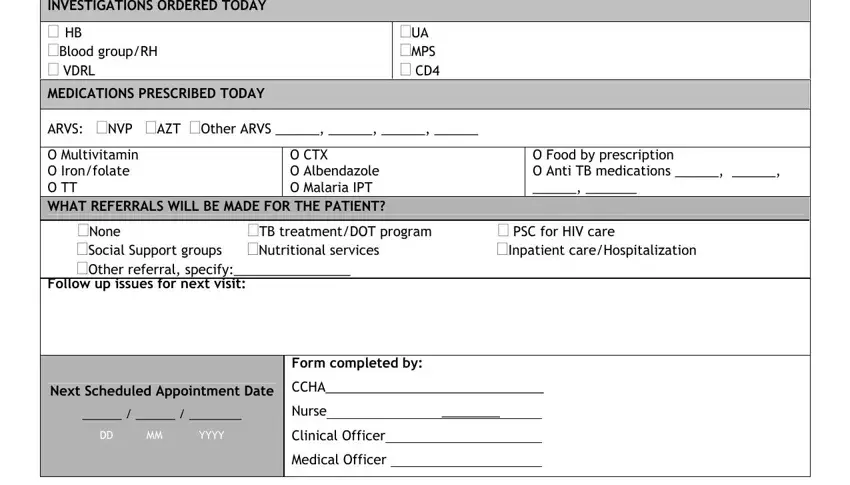
Finish by reviewing the next sections and filling them in as required: INVESTIGATIONS ORDERED TODAY HB, UA MPS CD, ARVS NVP AZT Other ARVS, O Multivitamin O Ironfolate O TT, O CTX O Albendazole O Malaria IPT, O Food by prescription O Anti TB, None, TB treatmentDOT program, PSC for HIV care, Social Support groups Nutritional, Next Scheduled Appointment Date, CCHA, Nurse, Form completed by, and DD MM YYYY.
Step 3: After you have hit the Done button, your file should be readily available transfer to any kind of gadget or email address you identify.
Step 4: Be sure to make as many copies of your document as you can to stay away from potential issues.
