
Using the online PDF tool by FormsPal, you are able to fill in or alter prime therapeutics pa form here and now. Our team is dedicated to giving you the best possible experience with our editor by constantly adding new functions and enhancements. With these updates, using our editor gets easier than ever before! This is what you will need to do to get going:
Step 1: Click the "Get Form" button above. It is going to open our pdf tool so that you can begin completing your form.
Step 2: With our online PDF file editor, you could accomplish more than just fill in blank form fields. Edit away and make your docs seem faultless with customized text incorporated, or adjust the file's original content to excellence - all that comes with an ability to insert just about any graphics and sign the document off.
As for the fields of this specific document, here's what you want to do:
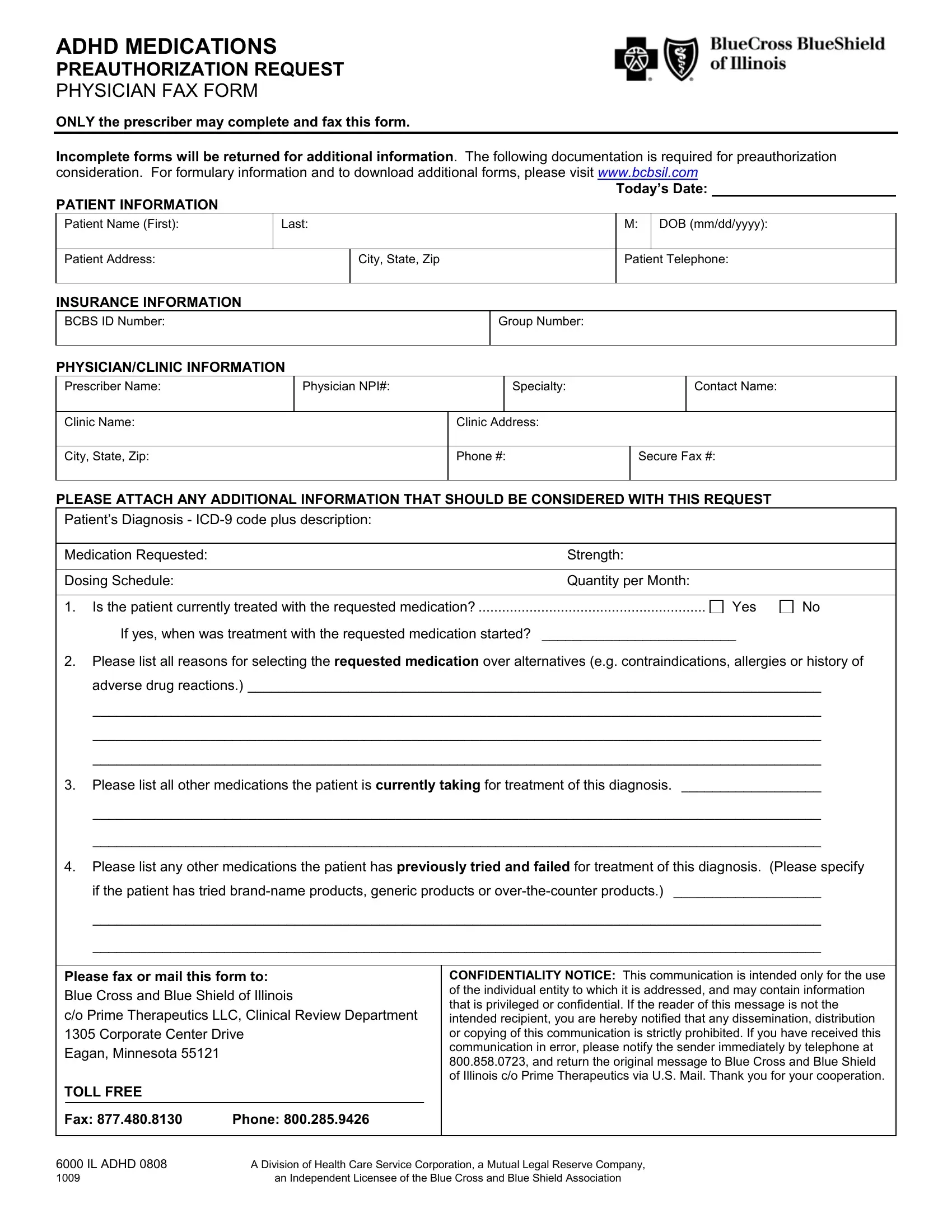
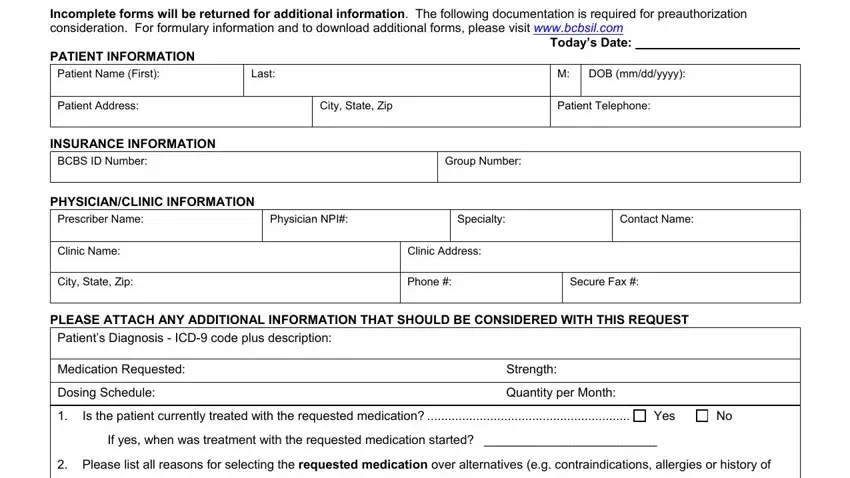
1. When submitting the prime therapeutics pa form, ensure to complete all of the important blank fields within the corresponding part. This will help to facilitate the work, which allows your details to be processed without delay and appropriately.
Step 3: Prior to finalizing the document, it's a good idea to ensure that form fields have been filled in as intended. Once you confirm that it's good, click on “Done." Make a 7-day free trial subscription at FormsPal and gain immediate access to prime therapeutics pa form - with all changes saved and available inside your FormsPal cabinet. FormsPal is dedicated to the privacy of all our users; we ensure that all information used in our system is protected.