Our PDF editor makes completing files simple and easy. It is very an easy task to enhance the [FORMNAME] document. Stick to these particular steps to be able to achieve this:
Step 1: Click the button "Get form here" to open it.
Step 2: So, you can start modifying your Print Va Form 21 4192. Our multifunctional toolbar is at your disposal - add, erase, transform, highlight, and perform similar commands with the text in the document.
Feel free to type in the next details to complete the Print Va Form 21 4192 PDF:
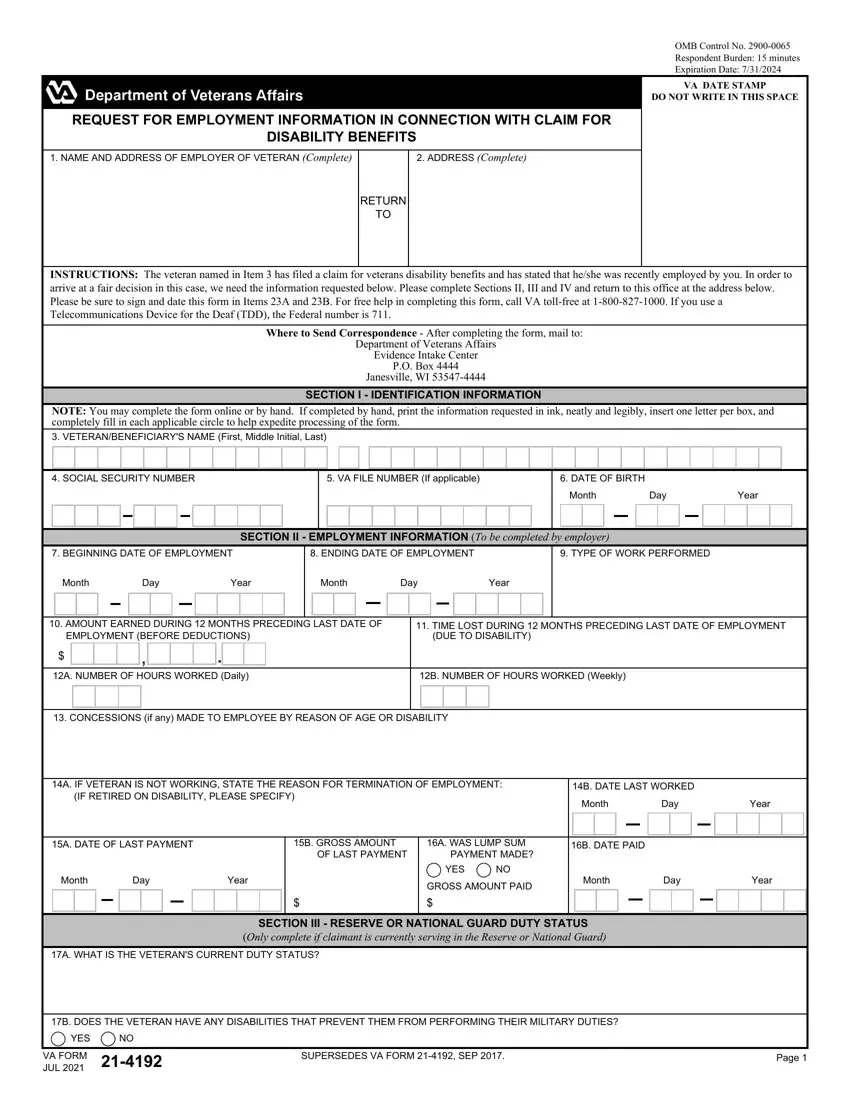
Jot down the data in the Month, Day, Year, Month, Day, Year, AMOUNT EARNED DURING MONTHS, TIME LOST DURING MONTHS, EMPLOYMENT BEFORE DEDUCTIONS, DUE TO DISABILITY, A NUMBER OF HOURS WORKED Daily, B NUMBER OF HOURS WORKED Weekly, CONCESSIONS if any MADE TO, A IF VETERAN IS NOT WORKING STATE, and B DATE LAST WORKED field.
Write down the necessary particulars in A WHAT IS THE VETERANS CURRENT, B DOES THE VETERAN HAVE ANY, YES, VA FORM JUL, SUPERSEDES VA FORM SEP, and Page segment.

In the box VETERANS SOCIAL SECURITY NO, IS VETERAN RECEIVING OR ENTITLED, SECTION IV INFORMATION ON BENEFIT, YES, If Yes complete Items through C, TYPE OF BENEFIT, GROSS MONTHLY AMOUNT OF BENEFIT, A DATE BENEFIT BEGAN, B DATE FIRST PAYMENT ISSUED, C DATE BENEFIT WILL STOP If known, Month, Day, Year, Month, and Day, describe the rights and responsibilities of the parties.
End by reviewing the next sections and submitting the pertinent details: PENALTY The law provides severe, VA will not disclose information, PRIVACY ACT NOTICE or Title Code, We need this information to, RESPONDENT BURDEN Code allows us, VA FORM JUL, and Page.
Step 3: Select the "Done" button. Next, it is possible to transfer the PDF document - save it to your device or deliver it via email.
Step 4: Just be sure to create as many duplicates of your document as you can to prevent possible issues.
