
You'll find nothing difficult about completing the printable medication card once you open our PDF editor. By taking these simple actions, you will definitely get the prepared PDF document within the minimum time period you can.
Step 1: Choose the orange "Get Form Now" button on the following page.
Step 2: You will find each of the options that you can take on your file once you've got entered the printable medication card editing page.
The following sections will create the PDF document that you will be filling in:
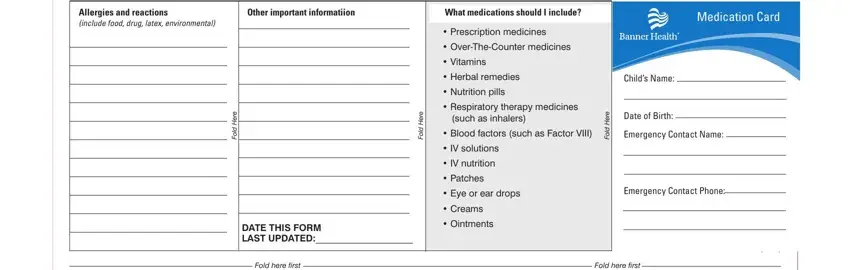
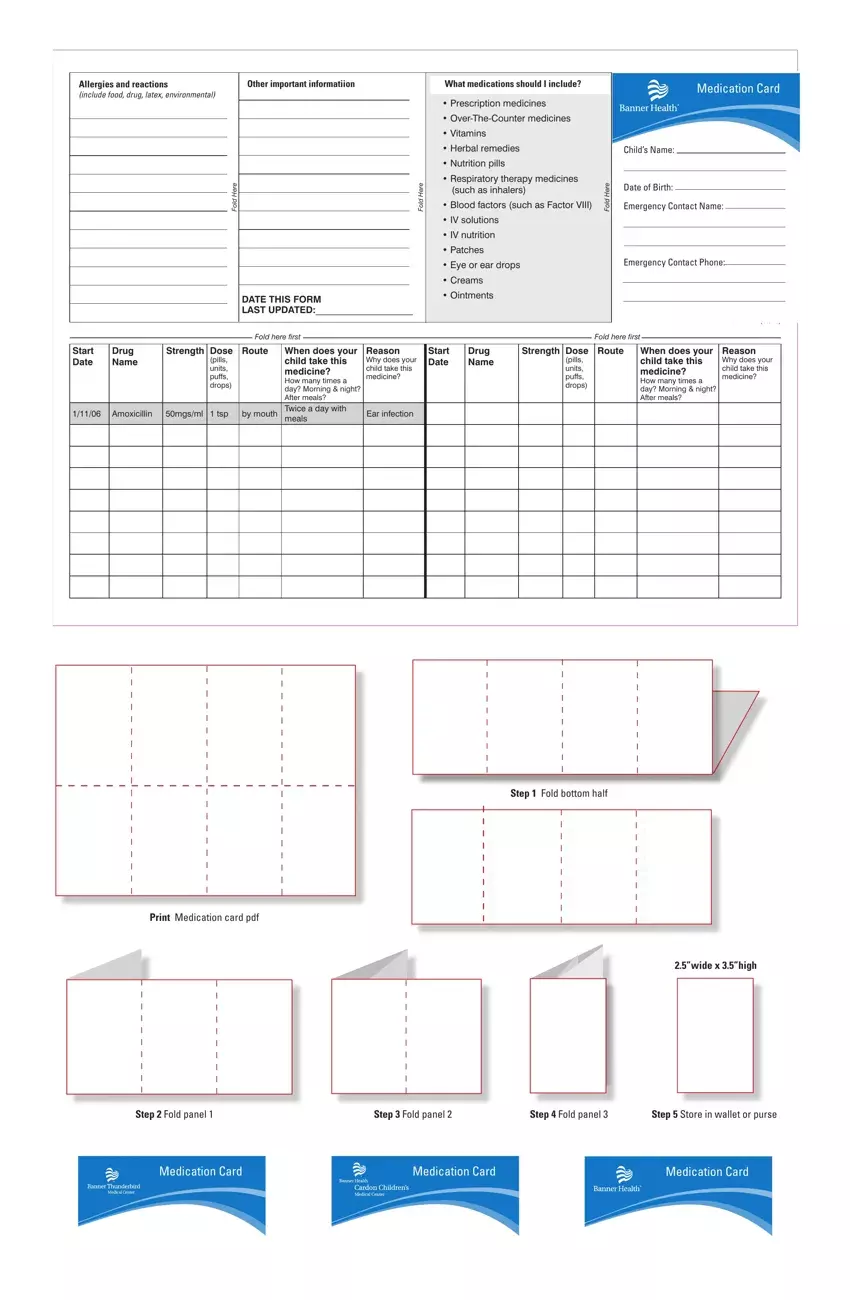
Write the requested particulars in the pills units puffs drops, Amoxicillin, mgsml tsp, by mouth, When does your child take this, Ear infection, pills units puffs drops, and When does your child take this part.
Step 3: Choose the Done button to ensure that your finalized file is available to be transferred to every device you prefer or sent to an email you indicate.
Step 4: To prevent yourself from probable upcoming complications, take the time to possess no less than a couple of copies of each separate file.
