In the realm of psychiatric care, maintaining accurate and thorough documentation is not just a procedural necessity but also a cornerstone of effective treatment planning and patient safety. The Psychiatric Progress Note form, designed exclusively for use by psychiatrists or advanced practice nurses with prescribing privileges in a psychopharmacology service, embodies this principle. This detailed form covers several crucial areas of patient care, including identifying information, interim history, mental status, medication adherence, side effects, allergic reactions, changes in medical status, and more. It ensures the systematic tracking of a patient's progress, response to medication, and any modification in treatment strategy, thereby playing a pivotal role in the continuum of care. By documenting therapeutic interventions—from psychotherapy to medication management—and summarizing laboratory test results, the form facilitates a comprehensive review of the patient's journey. Moreover, the emphasis on informed consent and detailed instructions underscores the commitment to patient autonomy and education. This precise approach to documentation not only aids in monitoring the efficacy of interventions but also ensures a high standard of care through clear communication and accountability.
| Question | Answer |
|---|---|
| Form Name | Psychiatric Progress Note |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | psychiatric progress note pdf, outpatient psychiatry note template, psychiatric documentation templates, psychiatry note template |

M S D P S T A N D A R D I Z E D D O C U M E N T A T I O N T R A I N I N G M A N U A L
Psychiatry/Medication Progress Note
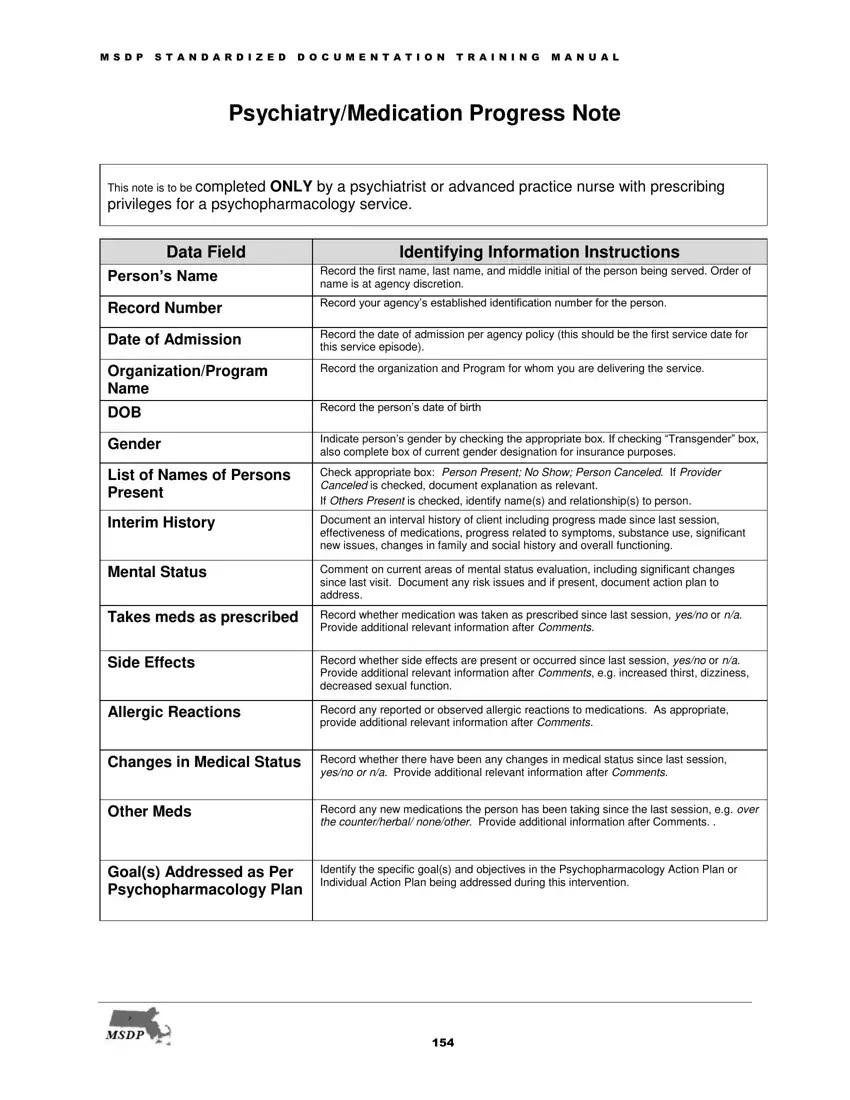
This note is to be completed ONLY by a psychiatrist or advanced practice nurse with prescribing privileges for a psychopharmacology service.
Data Field |
|
|
Identifying Information Instructions |
|
Person’s Name |
|
|
Record the first name, last name, and middle initial of the person being served. Order of |
|
|
|
name is at agency discretion. |
|
|
|
|
|
|
|
|
|
|
|
|
Record Number |
|
|
Record your agency’s established identification number for the person. |
|
|
|
|
|
|
|
|
|
|
|
Date of Admission |
|
|
Record the date of admission per agency policy (this should be the first service date for |
|
|
|
this service episode). |
|
|
|
|
|
|
|
|
|
|
|
|
Organization/Program |
|
|
Record the organization and Program for whom you are delivering the service. |
|
Name |
|
|
|
|
|
|
|
|
|
DOB |
|
|
Record the person’s date of birth |
|
|
|
|
|
|
|
|
|
|
|
Gender |
|
|
Indicate person’s gender by checking the appropriate box. If checking “Transgender” box, |
|
|
|
also complete box of current gender designation for insurance purposes. |
|
|
|
|
|
|
|
|
|
|
|
|
List of Names of Persons |
|
|
Check appropriate box: Person Present; No Show; Person Canceled. If Provider |
|
Present |
|
|
Canceled is checked, document explanation as relevant. |
|
|
|
If Others Present is checked, identify name(s) and relationship(s) to person. |
|
|
|
|
|
|
|
|
|
|
|
|
Interim History |
|
|
Document an interval history of client including progress made since last session, |
|
|
|
|
effectiveness of medications, progress related to symptoms, substance use, significant |
|
|
|
|
new issues, changes in family and social history and overall functioning. |
|
|
|
|
|
|
Mental Status |
|
|
Comment on current areas of mental status evaluation, including significant changes |
|
|
|
|
since last visit. Document any risk issues and if present, document action plan to |
|
|
|
|
address. |
|
|
|
|
|
|
Takes meds as prescribed |
|
|
Record whether medication was taken as prescribed since last session, yes/no or n/a. |
|
|
|
|
Provide additional relevant information after Comments. |
|
|
|
|
|
|
Side Effects |
|
|
Record whether side effects are present or occurred since last session, yes/no or n/a. |
|
|
|
|
Provide additional relevant information after Comments, e.g. increased thirst, dizziness, |
|
|
|
|
decreased sexual function. |
|
|
|
|
|
|
Allergic Reactions |
|
|
Record any reported or observed allergic reactions to medications. As appropriate, |
|
|
|
|
provide additional relevant information after Comments. |
|
|
|
|
|
|
Changes in Medical Status |
|
|
Record whether there have been any changes in medical status since last session, |
|
|
|
|
yes/no or n/a. Provide additional relevant information after Comments. |
|
|
|
|
|
|
Other Meds |
|
|
Record any new medications the person has been taking since the last session, e.g. over |
|
|
|
|
the counter/herbal/ none/other. Provide additional information after Comments. . |
|
|
|
|
|
|
Goal(s) Addressed as Per |
|
|
Identify the specific goal(s) and objectives in the Psychopharmacology Action Plan or |
|
Psychopharmacology Plan |
|
|
Individual Action Plan being addressed during this intervention. |
|
|
|
|
|
|
|
|
|
|
|
154

M S D P S T A N D A R D I Z E D D O C U M E N T A T I O N T R A I N I N G M A N U A L
Therapeutic Interventions |
|
|
Check one or more of the types of interventions delivered in the session: |
Delivered in Session |
|
|
Psychotherapy, Counseling/Coaching, Collaborative Medication Management, |
|
|
Collaborative Medication Education/Symptom/Illness Management, Injections, Physical |
|
|
|
|
|
|
|
|
Assessment, Coordination of Care. For additional interventions utilized check other. |
|
|
|
Describe the content of the interventions. If any |
|
|
|
psychotic is prescribed it is suggested that the |
|
|
|
carefully documented. |
|
|
|
|
Response to Intervention |
|
|
Document person’s response to intervention(s) delivered in the session and person’s |
Delivered in Session and |
|
|
progress towards goals and objectives. If no progress is made over time, this section |
|
|
should also address changes in strategy to produce positive change in the person. |
|
Progress Toward Goals |
|
|
|
|
|
|
|
and Objectives |
|
|
|
|
|
|
|
Lab Tests Ordered |
|
|
Summarize key laboratory test results received and reviewed. Check appropriate box to |
|
|
|
indicate whether key laboratory test results were ordered or, reviewed (with person). If |
|
|
|
lab results were not received, describe action to be taken to obtain results. |
|
|
|
|
AIMS Findings |
|
|
If AIMS (Abnormal Involuntary Movement Scale) test was administered, document |
|
|
findings. |
|
|
|
|
|
|
|
|
|
Height/Weight/BMI |
|
|
Record information pertaining to person’s height, weight, body mass index, blood |
Blood Pressure/VS |
|
|
pressure, and vital signs as relevant. Document if there has been communication |
|
|
between the prescriber and the PCP. Provide additional relevant information as |
|
|
|
|
appropriate. |
|
|
|
|
Diagnosis |
|
|
Document whether the person’s diagnosis has changed or not. If diagnosis has |
|
|
|
changed, check yes and proceed to Comprehensive Assessment Update form. |
Data Field |
|
|
Medication Orders Today |
None Prescribed |
|
|
Check box if no medications are prescribed today. If so, proceed to Next Appointment |
|
|
|
data field. |
Rationale for Changes in |
|
|
Document rationale for any medication changes. For each medication prescribed, |
Medications |
|
|
indicate if the medication is renewed(renew) /changed, newly prescribed (new) or |
|
|
discontinued (D/C). Write the name of the medication (med), dosage (dose), frequency |
|
|
|
|
|
|
|
|
(frequency), # of Days, quantity (qty), and number of refills (refills) prescribed. |
|
|
|
For each new medication prescribed, the person should be given information about |
|
|
|
medication risks and benefits. Check the appropriate box indicating whether person has |
|
|
|
given “informed consent”, i.e. demonstrated an understanding of medication’s risks and |
|
|
|
benefits. Documentation of “Informed Consent” is mandatory. If the person does not |
|
|
|
demonstrate an understanding of the risks and benefits, then the prescriber should |
|
|
|
indicate in the Instructions /Comments Section what steps should be taken. |
|
|
|
This section should not be a substitute for a complete listing of medications. |
|
|
|
|
Instructions/Comments, as |
|
|
Document any additional relevant instructions or |
applicable: |
|
|
|
|
|
|
|
Next Appointment |
|
|
Document time frame when the person should return to see the prescriber. |
|
|
|
|
MD/DO/APN (Print Name) |
|
|
Legibly print the MD/DO/APN’s name. |
|
|
|
|
MD/DO/APN Signature & |
|
|
Legibly record provider’s signature, credentials and date. |
Credentials |
|
|
|
|
|
|
|
Supervisor - Print |
|
|
If required, legibly print name of supervisor, credentials and date. |
Name/Credential (If |
|
|
|
needed) |
|
|
|
|
|
|
|
Supervisor - Signature (If |
|
|
If required, legible record Supervisor Signature. |
needed) |
|
|
|
|
|
|
|
155
