This PDF editor enables you to fill in documents. You don't have to undertake much to change serogroups files. Basically stick to the next steps.
Step 1: Step one will be to click the orange "Get Form Now" button.
Step 2: After you've entered the titers editing page you may discover the different actions you'll be able to perform with regards to your template from the upper menu.
The particular sections will make up the PDF document:
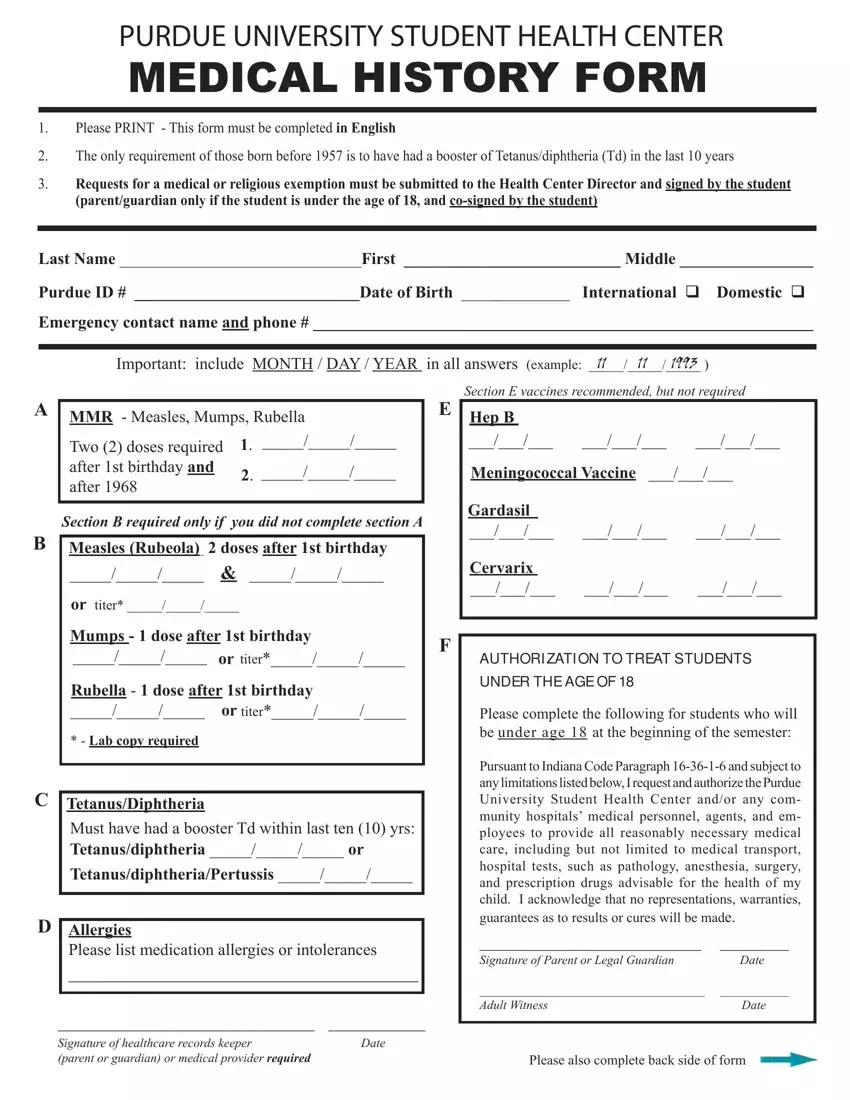
The application will require you to complete the Two doses required after st, Meningococcal Vaccine, Hep B, Section B required only if you did, Measles Rubeola doses after st, or titer, Gardasil, Cervarix, Mumps dose after st birthday, F titer, Rubella dose after st birthday, titer, Lab copy required, TetanusDiphtheria Must have had a, and AUTHORI ZATI ON TO TREAT STUDENTS field.
The program will ask you for data to instantly complete the section TetanusDiphtheria Must have had a, TetanusdiphtheriaPertussis, Allergies Please list medication, Signature of healthcare records, Pursuant to Indiana Code Paragraph, Signature of Parent or Legal, Adult Witness Date, and Please also complete back side of.
The By signing below I acknowledge, Student or parent if student is, I NSURANCE I NFORM ATI ON, For assistance in fi ling insurance, Name of primary policyholder, Male Female, By signing below I acknowledge, Parent, Date, Student, and Date section is the place to insert the rights and obligations of both parties.
Step 3: Select the Done button to ensure that your finalized file can be exported to any type of gadget you decide on or sent to an email you indicate.
Step 4: It can be better to save duplicates of your document. You can be sure that we will not disclose or view your particulars.
