
When using the online tool for PDF editing by FormsPal, you can easily complete or change Qme Form 105 here. To have our tool on the cutting edge of practicality, we aim to put into operation user-oriented features and enhancements on a regular basis. We are at all times grateful for any suggestions - assist us with reshaping the way you work with PDF forms. All it takes is a few simple steps:
Step 1: Press the orange "Get Form" button above. It will open up our editor so you can start filling out your form.
Step 2: With this advanced PDF file editor, it is possible to do more than just complete blanks. Express yourself and make your documents look high-quality with custom text added, or optimize the file's original input to perfection - all that accompanied by an ability to incorporate stunning images and sign the PDF off.
Filling out this form will require attentiveness. Make certain every single blank is done correctly.
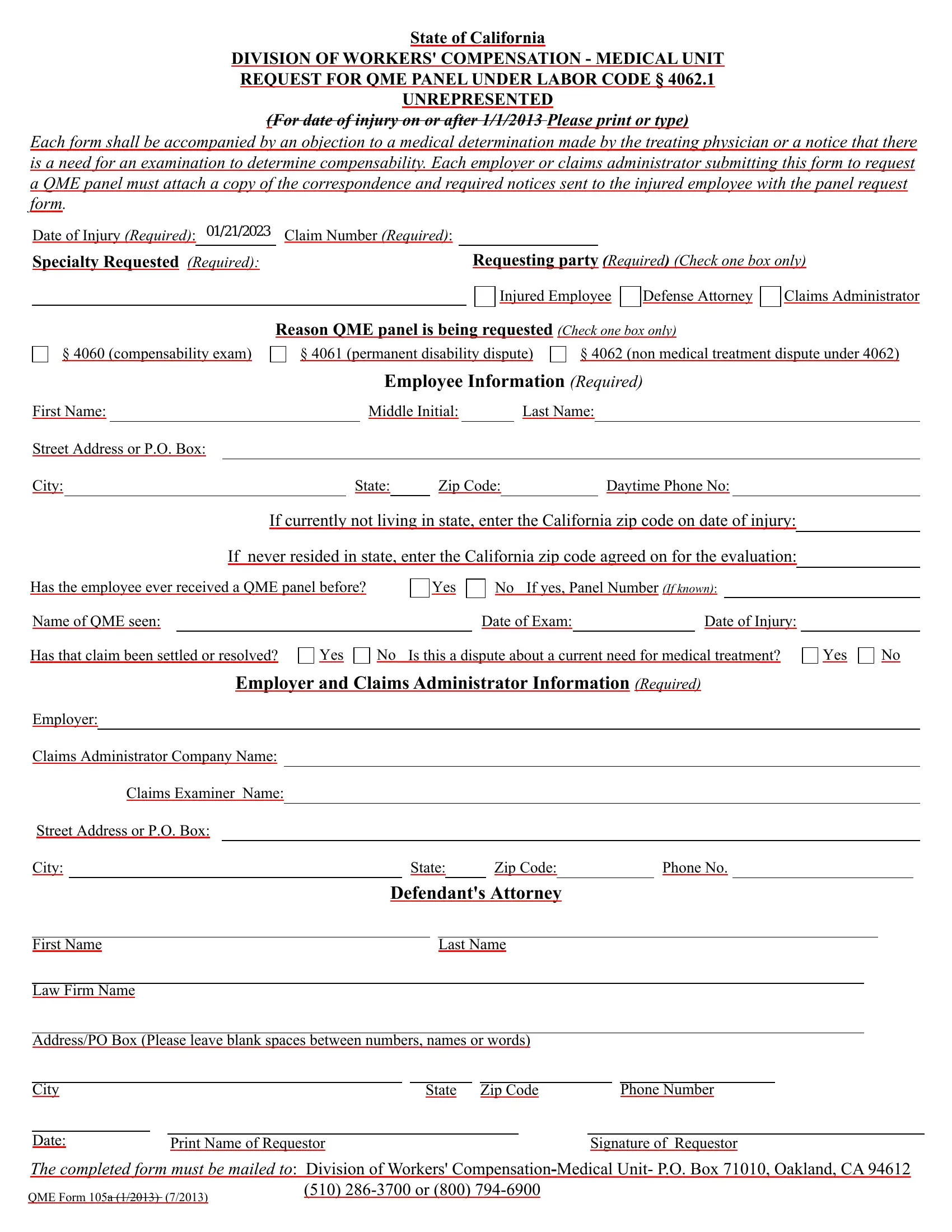
1. Whenever filling out the Qme Form 105, ensure to complete all of the important blanks within the corresponding section. This will help expedite the work, allowing your information to be handled efficiently and appropriately.
2. Once your current task is complete, take the next step – fill out all of these fields - Name of QME seen, Date of Exam, Date of Injury, Has that claim been settled or, Yes, Is this a dispute about a current, Yes, Employer and Claims Administrator, Employer, Claims Administrator Company Name, Claims Examiner Name, Street Address or PO Box, City, State, and Zip Code with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
Many people often make mistakes while filling in Street Address or PO Box in this area. You need to go over whatever you enter right here.
3. In this stage, check out City, Date, State, Zip Code, Phone Number, Print Name of Requestor, Signature of Requestor, and The completed form must be mailed. Each of these will have to be filled in with greatest attention to detail.

4. The form's fourth part comes with these particular blanks to consider: I declare that I am a resident of, On I served this QME form the, or firm named below and by, depositing the sealed envelope, placing the sealed envelope for, placing the sealed envelope for, placing the sealed envelope for, personally delivering the sealed, Method of Service, Person or firm served, and Street Address.
5. And finally, this last segment is precisely what you will have to complete before closing the document. The fields in this case are the following: Method of Service, Method of Service, Method of Service, City, State, Zip Code, Person or firm served, Street Address, City, State, Zip Code, Person or firm served, Street Address, City, and State.
Step 3: Before moving forward, it's a good idea to ensure that all blank fields have been filled out right. Once you determine that it is good, click “Done." Get your Qme Form 105 when you sign up at FormsPal for a 7-day free trial. Conveniently get access to the pdf from your personal account, along with any modifications and changes being automatically kept! FormsPal is dedicated to the confidentiality of all our users; we make certain that all personal information going through our system remains protected.