
pa586 form can be completed online effortlessly. Simply use FormsPal PDF tool to complete the job quickly. In order to make our tool better and simpler to work with, we continuously design new features, taking into consideration feedback coming from our users. To get the ball rolling, take these simple steps:
Step 1: Just click on the "Get Form Button" at the top of this webpage to see our pdf editing tool. There you'll find all that is necessary to fill out your document.
Step 2: As soon as you access the editor, there'll be the document all set to be filled out. In addition to filling in various blanks, you may as well do several other things with the Document, specifically writing custom text, modifying the initial textual content, adding images, affixing your signature to the PDF, and much more.
With regards to the fields of this specific document, this is what you should do:
1. The pa586 form involves certain information to be entered. Ensure the subsequent blanks are finalized:
2. Once your current task is complete, take the next step – fill out all of these fields - SECTION II TO BE COMPLETED BY, HISTORY Complaints and history of, and DIAGNOSTIC STUDIES PREVIOUSLY with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
You can potentially make errors while completing your SECTION II TO BE COMPLETED BY, for that reason be sure to take another look prior to deciding to finalize the form.
3. The following step is all about PAGE - complete each of these empty form fields.
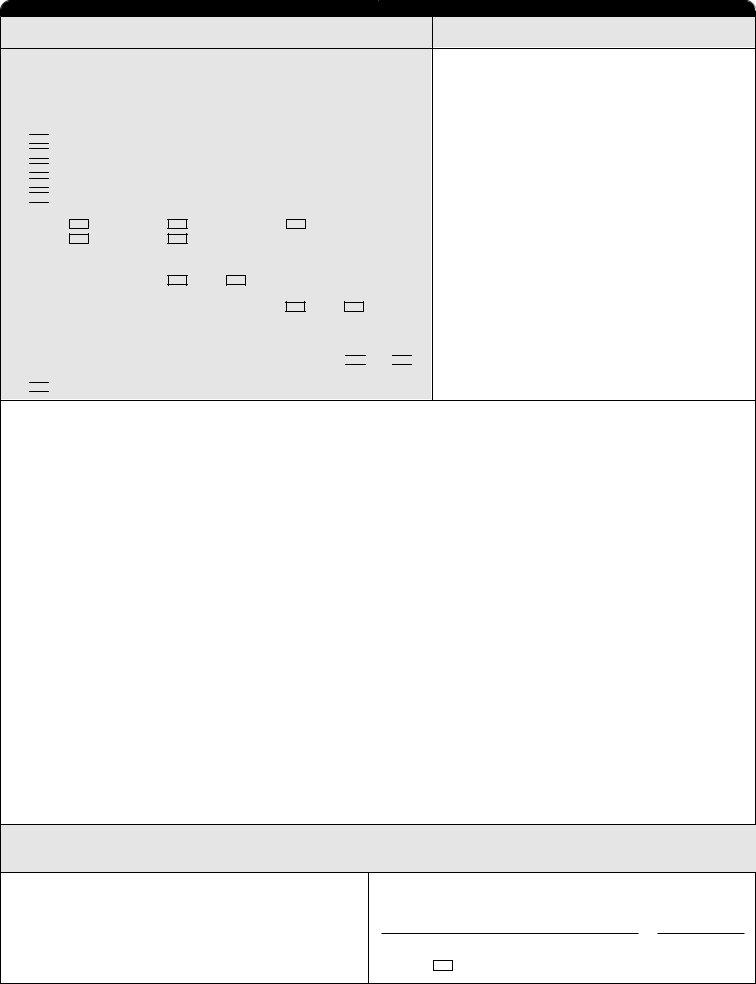
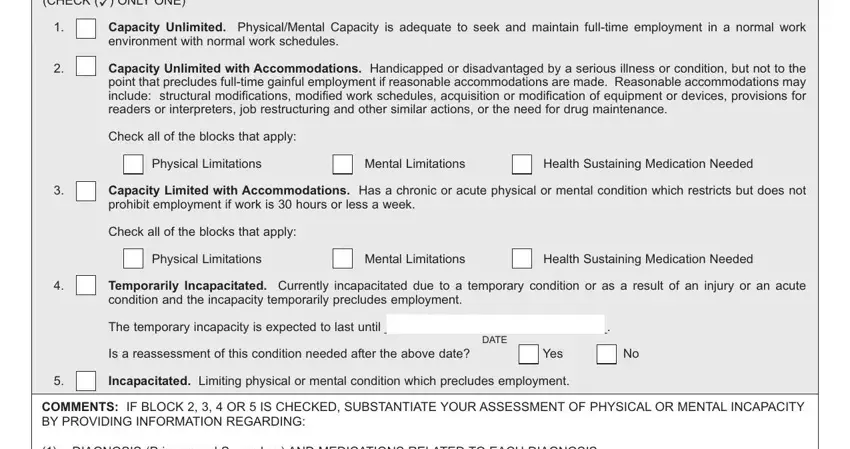
4. This next section requires some additional information. Ensure you complete all the necessary fields - PHYSICALMENTAL CAPACITY CHECK cid, Capacity Unlimited PhysicalMental, Capacity Unlimited with, Check all of the blocks that apply, Physical Limitations, Mental Limitations, Health Sustaining Medication Needed, Capacity Limited with, Check all of the blocks that apply, Physical Limitations, Mental Limitations, Health Sustaining Medication Needed, Temporarily Incapacitated, The temporary incapacity is, and DATE - to proceed further in your process!
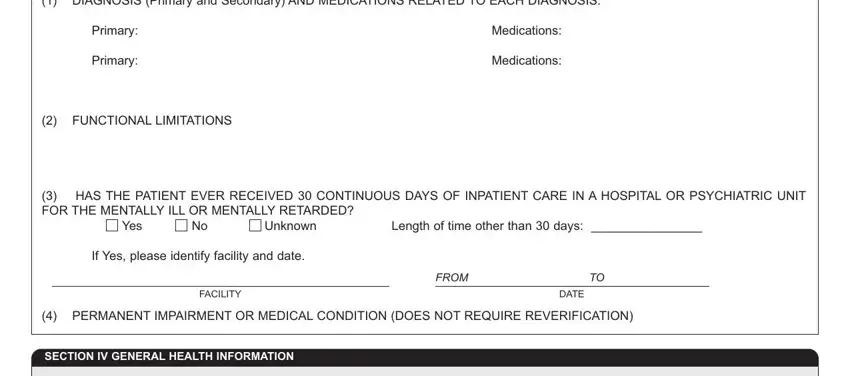
5. Last of all, the following last subsection is what you'll want to complete before closing the document. The blanks in question are the following: DIAGNOSIS Primary and Secondary, Primary, Primary, Medications, Medications, FUNCTIONAL LIMITATIONS, HAS THE PATIENT EVER RECEIVED, Yes, Unknown, Length of time other than days, If Yes please identify facility, FACILITY, FROM, DATE, and PERMANENT IMPAIRMENT OR MEDICAL.
Step 3: After double-checking your entries, hit "Done" and you're all set! Get hold of the pa586 form once you sign up for a free trial. Conveniently access the pdf form from your FormsPal cabinet, together with any edits and adjustments being automatically synced! At FormsPal, we endeavor to guarantee that all of your information is stored secure.