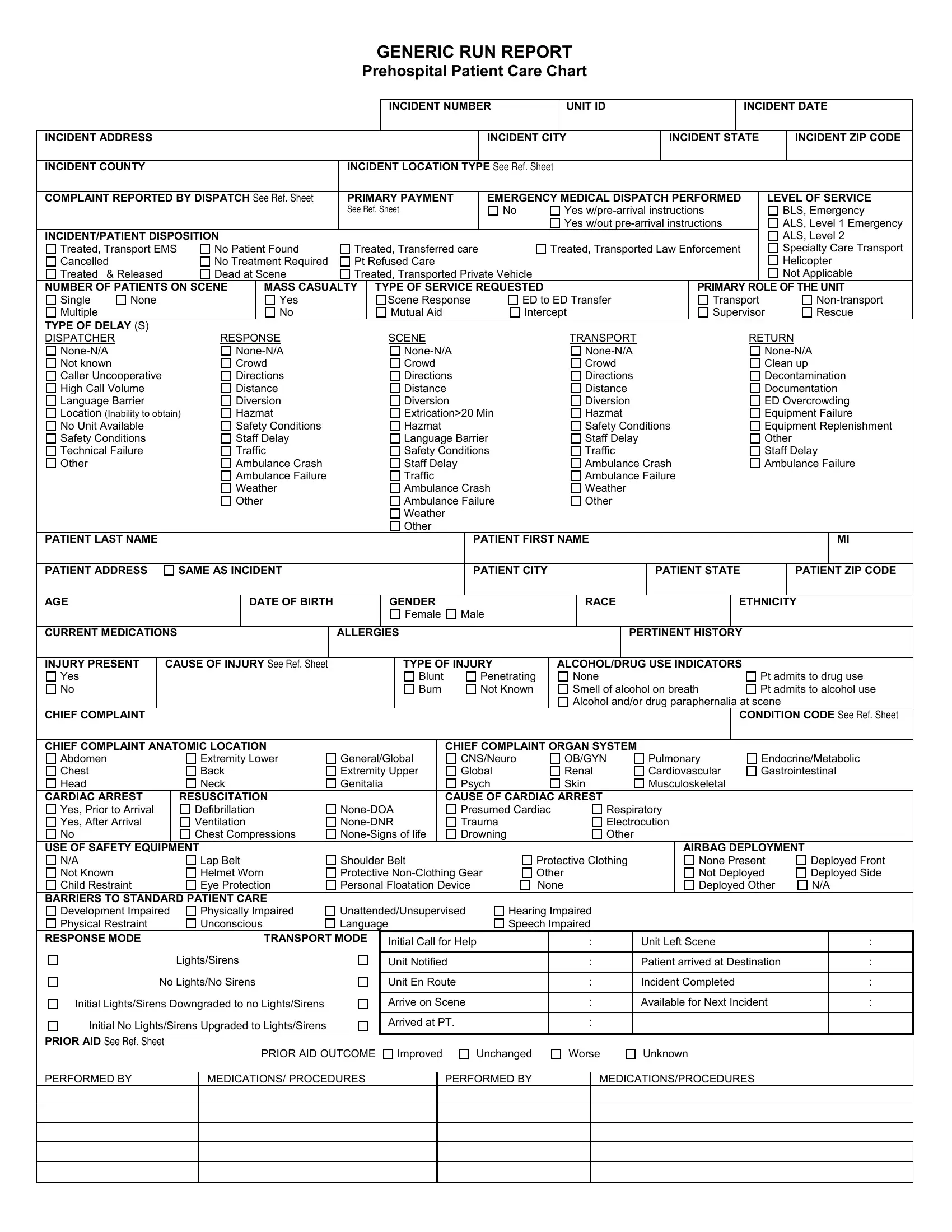
In the fast-paced world of emergency medical services (EMS), comprehensive documentation is crucial for patient care, legal accountability, and quality improvement. The Report Patient Care Chart form serves as a detailed record encompassing all aspects of EMS interventions from the incident call to the patient's outcome. This generic run report starts with basic incident identifiers, such as the number, address, and type of incident, alongside patient demographics including their name, age, and critical medical history. Distinct sections detail the emergency response, including the level of service provided, patient disposition, and any pertinent clinical information such as chief complaints, vital signs, medications administered, and procedures performed. The form also acknowledges the complexities encountered during emergency calls by recording potential barriers to care and specifying any prehospital patient care challenges, like high call volume or hazardous material presence. Furthermore, aspects like the use of safety equipment and the patient’s reaction to interventions are meticulously noted to ensure a comprehensive overview of the response efforts and outcomes. This document is essential for bridging the gap between pre-hospital and hospital care, ensuring continuity of care, and facilitating audits and feedback for EMS providers.
| Question | Answer |
|---|---|
| Form Name | Report Patient Care Chart Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | report form prehospital care, report care generic, ems run reports, report form prehospital patient |
GENERIC RUN REPORT
Prehospital Patient Care Chart
|
|
|
|
|
|
|
|
|
|
|
|
|
INCIDENT NUMBER |
|
|
|
UNIT ID |
|
|
|
|
|
|
INCIDENT DATE |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
INCIDENT ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INCIDENT CITY |
|
|
INCIDENT STATE |
|
|
INCIDENT ZIP CODE |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
INCIDENT COUNTY |
|
|
|
|
|
|
|
INCIDENT LOCATION TYPE SEE REF. SHEET |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
COMPLAINT REPORTED BY DISPATCH SEE REF. SHEET |
PRIMARY PAYMENT |
|
|
EMERGENCY MEDICAL DISPATCH PERFORMED |
LEVEL OF SERVICE |
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
SEE REF. SHEET |
|
|
|
No |
Yes |
|
BLS, Emergency |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes w/out |
|
ALS, Level 1 Emergency |
||||||||||||
INCIDENT/PATIENT DISPOSITION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ALS, Level 2 |
|||||||
Treated, Transport EMS |
No Patient Found |
Treated, Transferred care |
|
Treated, Transported Law Enforcement |
|
Specialty Care Transport |
||||||||||||||||||||||||||||||
Cancelled |
|
|
No Treatment Required |
Pt Refused Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Helicopter |
|||||||||||||
Treated |
& Released |
|
|
Dead at Scene |
Treated, Transported Private Vehicle |
|
|
|
|
|
|
|
|
|
|
|
|
Not Applicable |
||||||||||||||||||
NUMBER OF PATIENTS ON SCENE |
|
|
MASS CASUALTY |
TYPE OF SERVICE REQUESTED |
|
|
|
|
|
|
|
|
PRIMARY ROLE OF THE UNIT |
|||||||||||||||||||||||
Single |
None |
|
|
|
|
|
Yes |
|
|
|
Scene Response |
ED to ED Transfer |
|
|
|
|
Transport |
|
|
|||||||||||||||||
Multiple |
|
|
|
|
|
|
|
No |
|
|
|
Mutual Aid |
|
|
|
Intercept |
|
|
|
|
Supervisor |
|
Rescue |
|||||||||||||
TYPE OF DELAY (S) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
DISPATCHER |
|
|
RESPONSE |
|
|
|
SCENE |
|
|
|
|
|
|
TRANSPORT |
|
|
|
|
|
|
RETURN |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Not known |
|
|
|
Crowd |
|
|
|
|
Crowd |
|
|
|
|
|
|
|
Crowd |
|
|
|
|
|
|
|
Clean up |
|||||||||||
Caller Uncooperative |
|
|
|
Directions |
|
|
|
|
Directions |
|
|
|
|
|
|
|
Directions |
|
|
|
|
|
|
|
Decontamination |
|||||||||||
High Call Volume |
|
|
|
Distance |
|
|
|
|
Distance |
|
|
|
|
|
|
|
Distance |
|
|
|
|
|
|
|
Documentation |
|||||||||||
Language Barrier |
|
|
|
Diversion |
|
|
|
|
Diversion |
|
|
|
|
|
|
|
Diversion |
|
|
|
|
|
|
|
ED Overcrowding |
|||||||||||
Location (Inability to obtain) |
Hazmat |
|
|
|
|
Extrication>20 Min |
|
|
|
|
Hazmat |
|
|
|
|
|
|
|
Equipment Failure |
|||||||||||||||||
No Unit Available |
|
|
|
Safety Conditions |
|
|
|
|
Hazmat |
|
|
|
|
|
|
|
Safety Conditions |
Equipment Replenishment |
||||||||||||||||||
Safety Conditions |
|
|
|
Staff Delay |
|
|
|
|
Language Barrier |
|
|
|
|
Staff Delay |
|
|
|
|
|
|
|
Other |
||||||||||||||
Technical Failure |
|
|
|
Traffic |
|
|
|
|
Safety Conditions |
|
|
|
|
Traffic |
|
|
|
|
|
|
|
Staff Delay |
||||||||||||||
Other |
|
|
|
|
|
Ambulance Crash |
|
|
|
|
Staff Delay |
|
|
|
|
|
|
|
Ambulance Crash |
Ambulance Failure |
||||||||||||||||
|
|
|
|
|
|
Ambulance Failure |
|
|
|
|
Traffic |
|
|
|
|
|
|
|
Ambulance Failure |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
Weather |
|
|
|
|
Ambulance Crash |
|
|
|
|
Weather |
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
Other |
|
|
|
|
Ambulance Failure |
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weather |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT LAST NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT FIRST NAME |
|
|
|
|
|
|
|
|
|
|
MI |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
PATIENT ADDRESS |
|
|
SAME AS INCIDENT |
|
|
|
|
|
|
|
PATIENT CITY |
|
|
|
|
|
PATIENT STATE |
|
|
PATIENT ZIP CODE |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
AGE |
|
|
|
|
|
|
DATE OF BIRTH |
|
|
|
GENDER |
|
|
|
|
|
|
|
RACE |
|
|
|
|
|
|
ETHNICITY |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Female |
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
CURRENT MEDICATIONS |
|
|
|
|
|
ALLERGIES |
|
|
|
|
|
|
|
|
PERTINENT HISTORY |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
INJURY PRESENT |
|
CAUSE OF INJURY SEE REF. SHEET |
|
|
|
|
TYPE OF INJURY |
|
ALCOHOL/DRUG USE INDICATORS |
|
|
|
|
|||||||||||||||||||||||
Yes |
|
|
|
|
|
|
|
|
|
|
|
|
|
Blunt |
|
|
Penetrating |
|
None |
|
|
|
|
|
|
|
Pt admits to drug use |
|||||||||
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
Burn |
|
|
Not Known |
|
Smell of alcohol on breath |
Pt admits to alcohol use |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Alcohol and/or drug paraphernalia at scene |
|
|
|
|||||||||||
CHIEF COMPLAINT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONDITION CODE SEE REF. SHEET |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
CHIEF COMPLAINT ANATOMIC LOCATION |
|
|
|
|
|
CHIEF COMPLAINT ORGAN SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
Abdomen |
|
|
Extremity Lower |
General/Global |
|
CNS/Neuro |
OB/GYN |
|
Pulmonary |
Endocrine/Metabolic |
||||||||||||||||||||||||||
Chest |
|
|
|
|
Back |
|
|
|
|
Extremity Upper |
|
Global |
|
|
|
Renal |
|
Cardiovascular |
Gastrointestinal |
|||||||||||||||||
Head |
|
|
|
|
Neck |
|
|
|
|
Genitalia |
|
|
|
Psych |
|
|
|
Skin |
|
Musculoskeletal |
|
|
|
|
||||||||||||
CARDIAC ARREST |
|
|
RESUSCITATION |
|
|
|
|
|
CAUSE OF CARDIAC ARREST |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Yes, Prior to Arrival |
|
|
Defibrillation |
|
Presumed Cardiac |
|
Respiratory |
|
|
|
|
|||||||||||||||||||||||||
Yes, After Arrival |
|
|
Ventilation |
|
Trauma |
|
|
|
|
Electrocution |
|
|
|
|
||||||||||||||||||||||
No |
|
|
|
|
Chest Compressions |
|
Drowning |
|
Other |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
USE OF SAFETY EQUIPMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AIRBAG DEPLOYMENT |
||||||||||||
N/A |
|
|
|
|
Lap Belt |
Shoulder Belt |
|
|
|
Protective Clothing |
|
|
|
|
None Present |
|
Deployed Front |
|||||||||||||||||||
Not Known |
|
|
Helmet Worn |
Protective |
Other |
|
|
|
|
|
|
|
|
Not Deployed |
|
Deployed Side |
||||||||||||||||||||
Child Restraint |
|
|
Eye Protection |
Personal Floatation Device |
None |
|
|
|
|
|
|
|
|
Deployed Other |
|
N/A |
||||||||||||||||||||
BARRIERS TO STANDARD PATIENT CARE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Development Impaired |
Physically Impaired |
Unattended/Unsupervised |
Hearing Impaired |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Physical Restraint |
|
|
Unconscious |
Language |
|
|
|
Speech Impaired |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
RESPONSE MODE |
|
|
|
|
|
TRANSPORT MODE |
|
Initial Call for Help |
|
|
|
: |
|
|
Unit Left Scene |
|
|
|
: |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
Lights/Sirens |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
Unit Notified |
|
|
|
|
|
|
: |
|
|
Patient arrived at Destination |
|
: |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
No Lights/No Sirens |
|
|
|
Unit En Route |
|
|
|
|
|
|
: |
|
|
Incident Completed |
|
|
: |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
Initial Lights/Sirens Downgraded to no Lights/Sirens |
|
|
|
Arrive on Scene |
|
|
|
: |
|
|
Available for Next Incident |
|
: |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Initial No Lights/Sirens Upgraded to Lights/Sirens |
|
|
|
Arrived at PT. |
|
|
|
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
PRIOR AID SEE REF. SHEET |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
PRIOR AID OUTCOME Improved |
|
Unchanged |
Worse |
Unknown |
|
|
|
|
||||||||||||||||||||
PERFORMED BY
MEDICATIONS/ PROCEDURES
PERFORMED BY
MEDICATIONS/PROCEDURES