
You'll be able to fill out allianz request form effectively in our online PDF tool. We at FormsPal are devoted to making sure you have the absolute best experience with our editor by regularly presenting new functions and upgrades. Our tool is now a lot more useful as the result of the latest updates! At this point, editing PDF forms is easier and faster than ever. All it takes is several simple steps:
Step 1: Click on the "Get Form" button above on this webpage to get into our editor.
Step 2: Once you open the file editor, you will notice the document all set to be completed. Apart from filling out various blanks, you might also do some other things with the file, that is writing your own words, editing the initial text, adding illustrations or photos, putting your signature on the form, and a lot more.
This document will need some specific details; in order to ensure consistency, please take heed of the next tips:
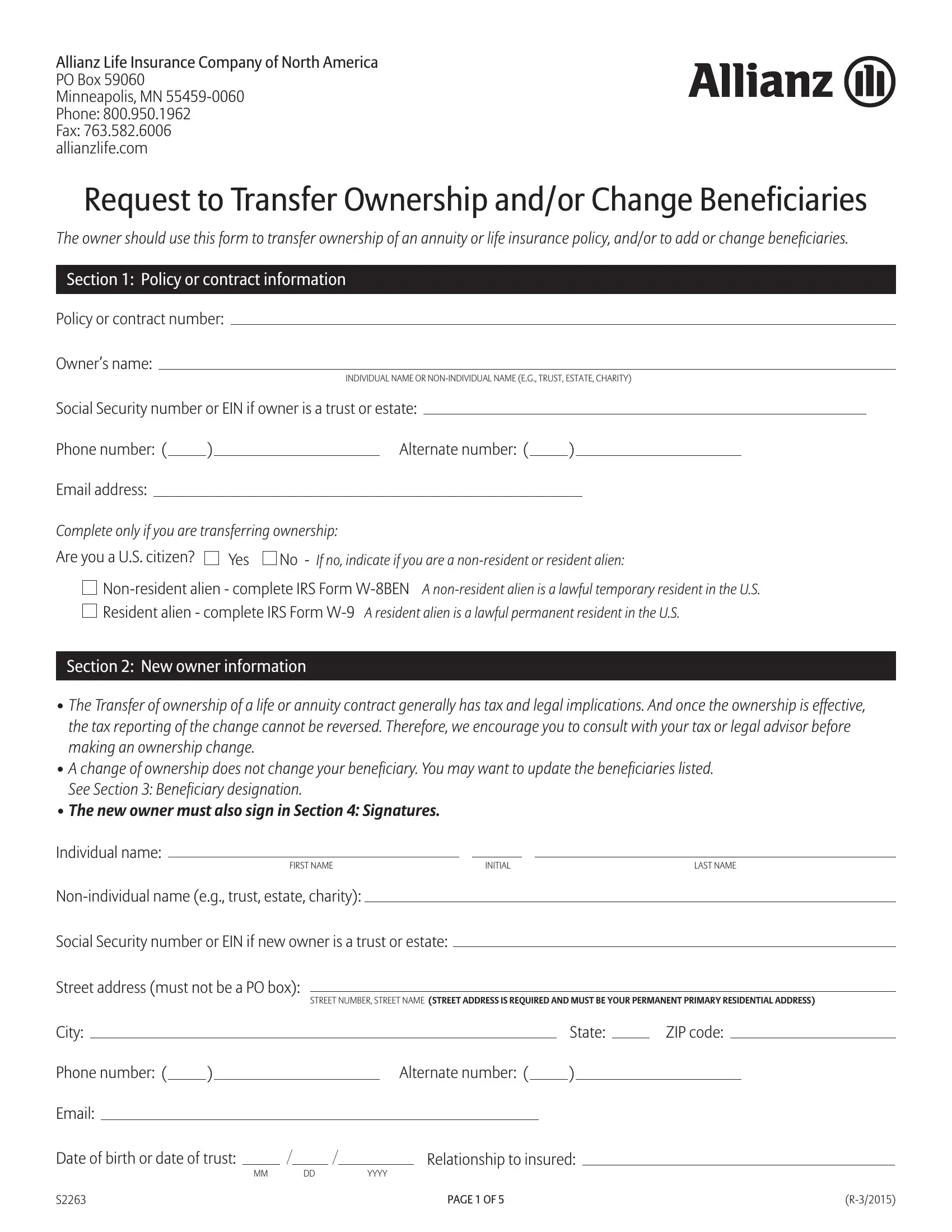
1. When filling in the allianz request form, be sure to complete all of the needed blank fields within its relevant area. This will help to hasten the work, allowing your information to be handled without delay and correctly.
2. Soon after filling out the previous part, head on to the subsequent step and fill out the essential details in these blank fields - The new owner must also sign in, Individual name, FIRST NAME, INITIAL, LAST NAME, Nonindividual name eg trust estate, Social Security number or EIN if, Street address must not be a PO box, STREET NUMBER STREET NAME STREET, City, State, ZIP code, Phone number, Alternate number, and Email.
Lots of people frequently get some points incorrect when filling out INITIAL in this area. You should definitely review everything you type in here.
3. Within this stage, have a look at Policy or contract number, Please write your policy or, Certification of Taxpayer, Under penalties of perjury I, The Taxpayer Identification, If the IRS has notified you that, I am not subject to backup, a I am exempt from backup, all interest or dividends or, c The IRS has notified me that I, I am a US person and, The Foreign Account Tax, reporting is correct, The IRS does not require your, and Additional documentation may be. Each one of these must be filled out with greatest accuracy.
4. You're ready to proceed to this next portion! Here you'll have all these Policy or contract number, Please write your policy or, Beneficiary Percentage, Select one, Primary, Contingent, Individual beneficiary name, FIRST NAME, INITIAL, LAST NAME, Nonindividual beneficiary name eg, Street address, City, STREET NUMBER STREET NAME, and State empty form fields to complete.
5. As a final point, this final section is precisely what you have to wrap up prior to submitting the form. The blank fields you're looking at are the next: Beneficiary Percentage, Select one, Primary, Contingent, Individual beneficiary name, FIRST NAME, INITIAL, LAST NAME, Nonindividual beneficiary name eg, Street address, City, STREET NUMBER STREET NAME, State, ZIP code, and Phone number.
Step 3: As soon as you've looked over the information in the file's blanks, click "Done" to complete your form at FormsPal. After creating a7-day free trial account here, you will be able to download allianz request form or email it at once. The PDF form will also be available via your personal account page with all your adjustments. FormsPal ensures your data confidentiality via a protected method that in no way saves or distributes any personal information provided. Feel safe knowing your docs are kept protected each time you work with our service!