



rks form 5 2020 can be filled in online easily. Simply use FormsPal PDF editor to do the job without delay. In order to make our tool better and more convenient to use, we consistently develop new features, with our users' suggestions in mind. Here is what you'd need to do to begin:
Step 1: Access the PDF form in our tool by clicking on the "Get Form Button" above on this page.
Step 2: With this online PDF editor, you're able to do more than just fill in blank fields. Try all of the features and make your docs seem high-quality with custom textual content put in, or fine-tune the original input to perfection - all that comes with the capability to insert any photos and sign the file off.
It will be an easy task to fill out the pdf using this detailed guide! Here is what you want to do:
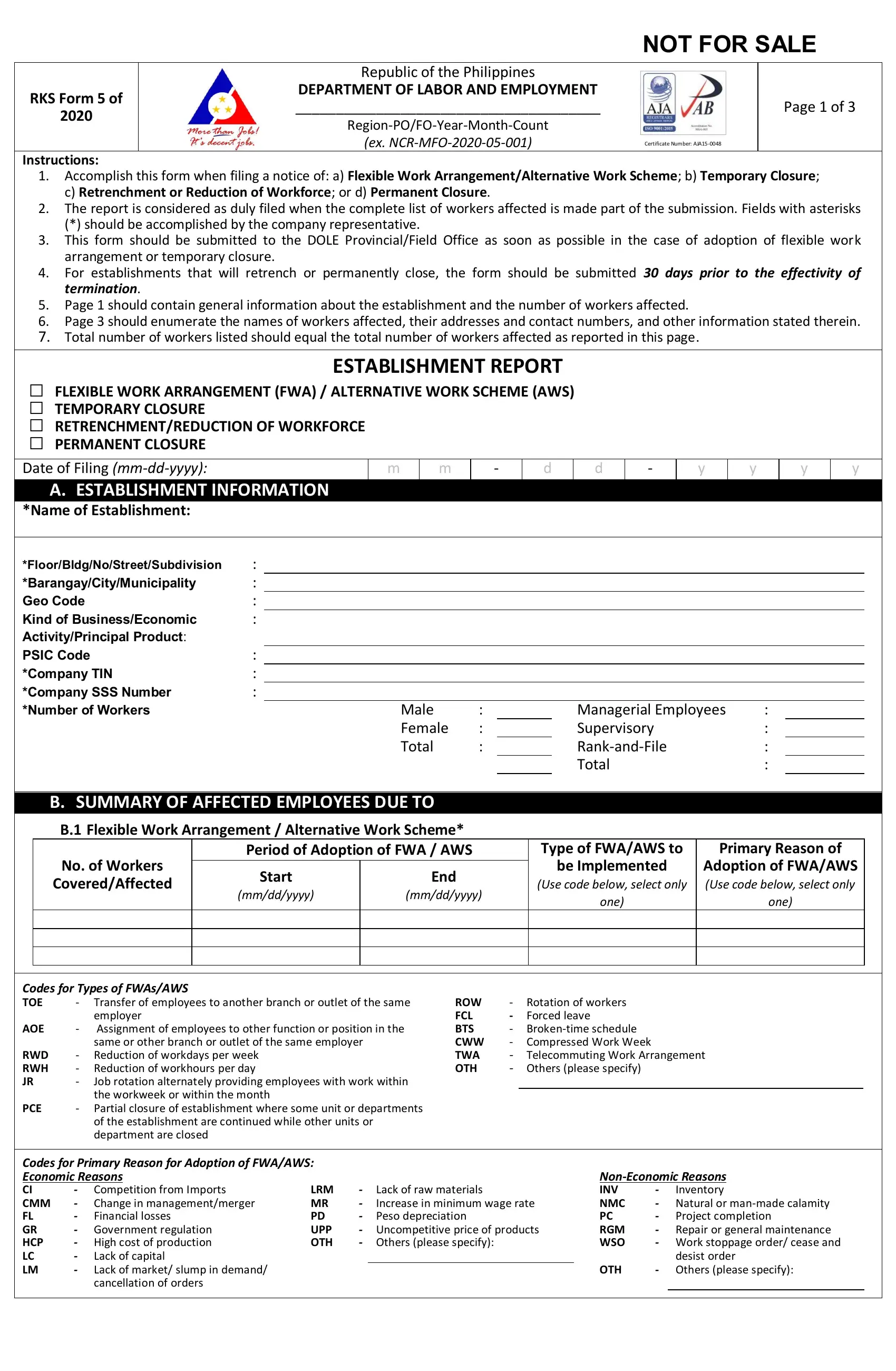
1. Begin completing the rks form 5 2020 with a selection of necessary blank fields. Gather all of the information you need and make sure there is nothing overlooked!
2. Soon after the last part is completed, go on to enter the relevant details in all these: Male Female Total, Managerial Employees Supervisory, Name of Establishment, B SUMMARY OF AFFECTED EMPLOYEES, B Flexible Work Arrangement, No of Workers, CoveredAffected, Period of Adoption of FWA AWS, Start, mmddyyyy, End, mmddyyyy, Type of FWAAWS to, Primary Reason of, and be Implemented.
3. Completing employer Assignment of employees, RWD RWH JR, Reduction of workdays per week, Job rotation alternately providing, ROW FCL BTS CWW TWA OTH, PCE, Partial closure of establishment, of the establishment are continued, Rotation of workers Forced leave, Competition from Imports Change in, Codes for Primary Reason for, Government regulation High, Lack of capital Lack of market, LRM MR PD UPP OTH, and Lack of raw materials Increase in is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
People who work with this PDF frequently make errors while filling out PCE in this area. Don't forget to go over whatever you type in right here.
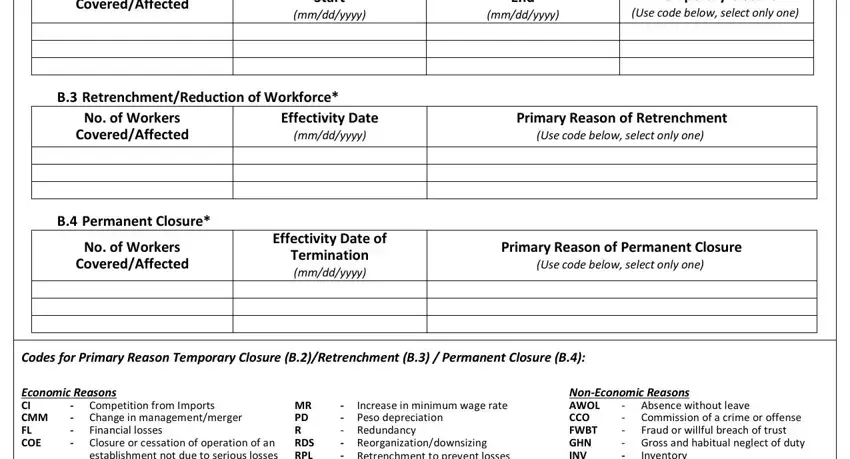
4. Your next section requires your details in the subsequent areas: CoveredAffected, Start, mmddyyyy, End, mmddyyyy, Primary Reason of Temporary Closure, Use code below select only one, B RetrenchmentReduction of, No of Workers, CoveredAffected, Effectivity Date, mmddyyyy, B Permanent Closure, No of Workers, and CoveredAffected. Just be sure you fill in all of the needed information to go forward.
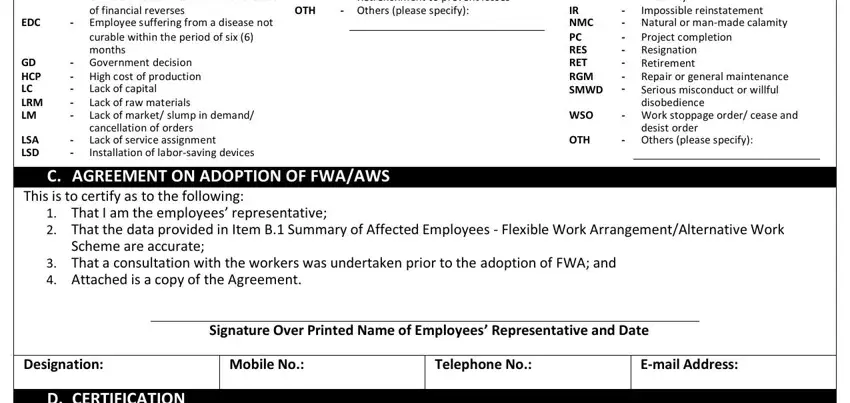
5. Lastly, this final portion is what you will need to wrap up prior to using the PDF. The blanks here include the next: Economic Reasons CI CMM FL COE EDC, months Government decision, MR Competition from Imports PD, Lack of capital Lack of raw, Peso depreciation Redundancy, NonEconomic Reasons AWOL CCO FWBT, Inventory Impossible reinstatement, Absence without leave Gross, Project completion Resignation, NMC, PC RES RET RGM SMWD WSO OTH, desist order, C AGREEMENT ON ADOPTION OF FWAAWS, This is to certify as to the, and That I am the employees.
Step 3: After going through your fields you have filled in, press "Done" and you are all set! Obtain your rks form 5 2020 when you sign up for a 7-day free trial. Readily get access to the pdf form within your FormsPal cabinet, with any modifications and adjustments being automatically preserved! At FormsPal.com, we endeavor to make certain that your information is kept secure.