
Using the online tool for PDF editing by FormsPal, you'll be able to complete or modify rsa 7 form billing right here. To make our editor better and simpler to utilize, we consistently design new features, with our users' suggestions in mind. With a few simple steps, you'll be able to begin your PDF journey:
Step 1: Simply click on the "Get Form Button" in the top section of this page to start up our pdf file editing tool. There you'll find all that is required to fill out your file.
Step 2: The editor helps you modify PDF documents in a range of ways. Improve it by writing any text, adjust original content, and put in a signature - all at your convenience!
Filling out this document calls for focus on details. Ensure every single field is completed properly.
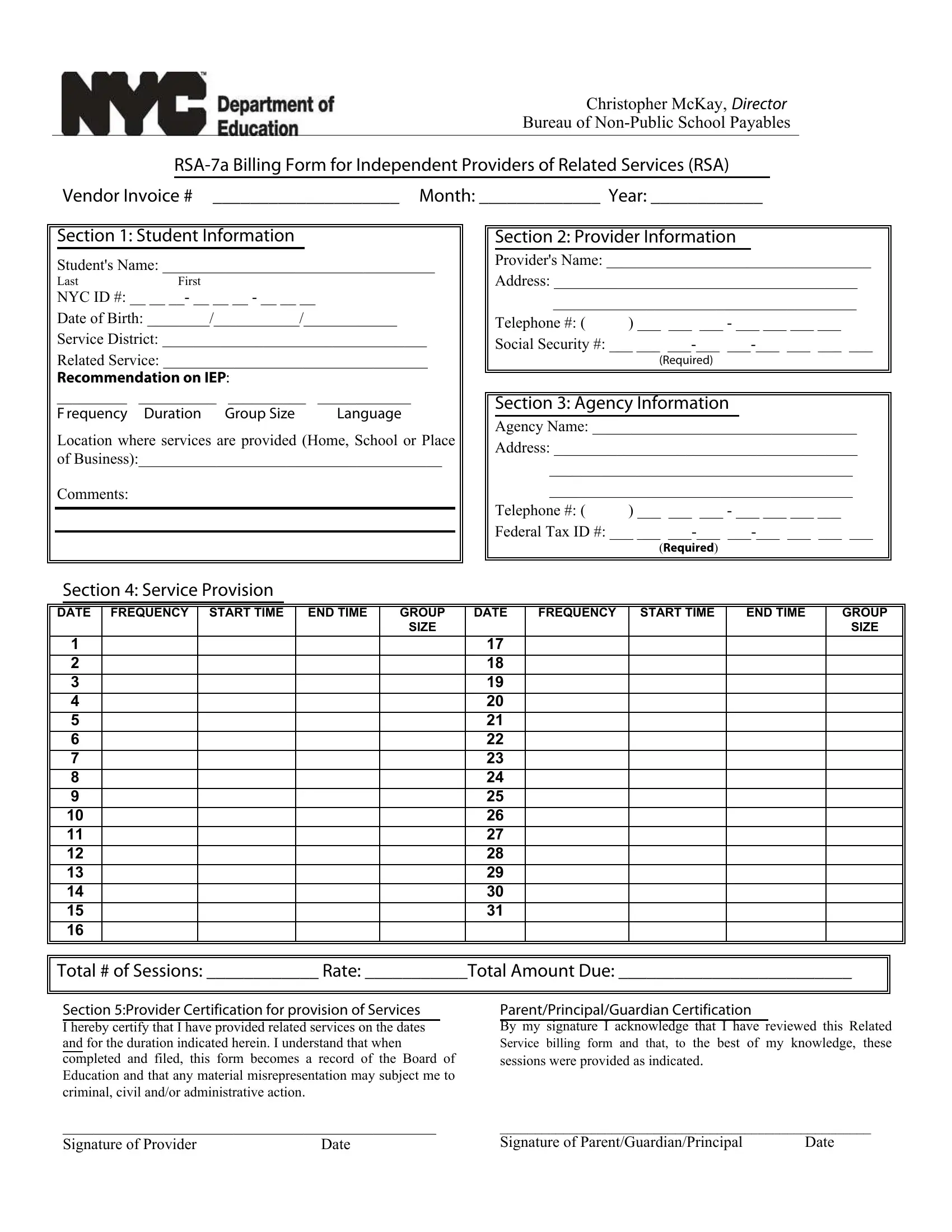
1. Begin completing your rsa 7 form billing with a group of essential fields. Get all of the necessary information and make sure absolutely nothing is overlooked!
2. After performing the last section, go on to the next step and fill in all required details in these fields - Total of Sessions Rate Total, Section Provider Certification for, ParentPrincipalGuardian, Signature of Provider Date, and Signature of.
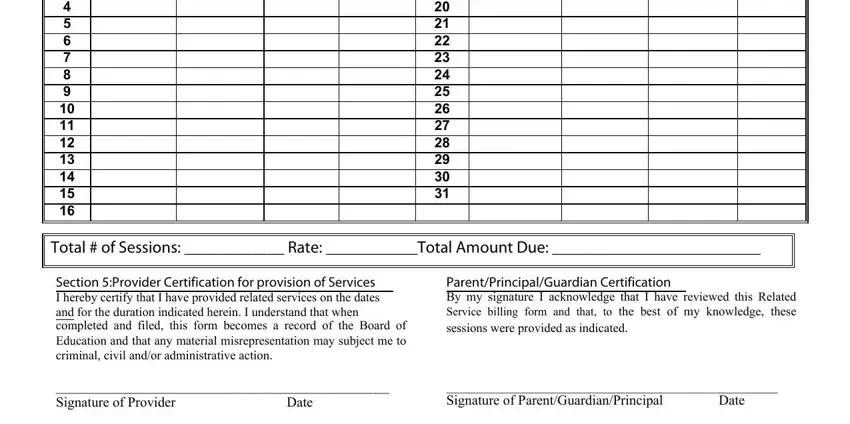
People often get some points incorrect while filling in Total of Sessions Rate Total in this section. You should re-examine what you enter right here.
Step 3: Before addressing the next step, you should make sure that all blanks have been filled in the proper way. The moment you confirm that it's fine, press “Done." Make a 7-day free trial plan at FormsPal and acquire direct access to rsa 7 form billing - which you may then make use of as you wish from your FormsPal account page. FormsPal is invested in the personal privacy of all our users; we make sure all personal information put into our tool is confidential.