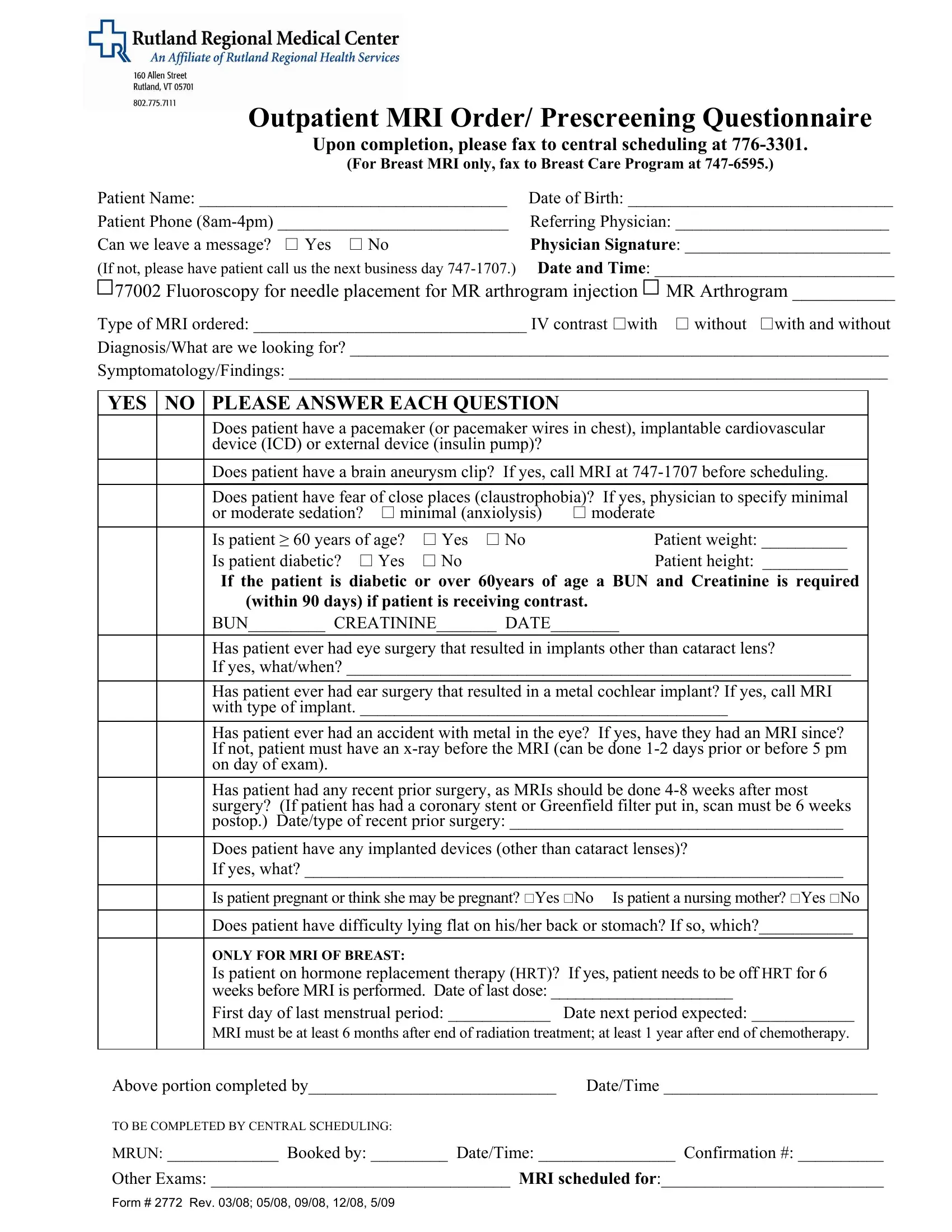
Ensuring a patient's safety and appropriate care during an MRI scan involves thorough preparation and screening. The Rutland 2772 form is a crucial document in this process, designed for outpatient MRI orders and prescreening questionnaires. Its use is a testament to the meticulous attention given to both medical and procedural aspects of MRI diagnostics. This form collects comprehensive patient information, including their name, date of birth, and contact details, ensuring clear identification and communication. Physicians are required to fill in specific details about the type of MRI ordered, highlighting whether IV contrast is needed and the diagnosis they are investigating. In addition to procedural details, the form meticulously screens for potential hazards or complications by inquiring about conditions like pacemakers, brain aneurysm clips, claustrophobia, and metal implants. Such precautions are vital, considering the strong magnetic fields used in MRI scans. The prescreening also considers the patient’s physical ability to undergo an MRI, asking about their ability to lie flat, and special considerations such as pregnancy or the patient being a nursing mother. For breast MRIs, the form inquires about hormone replacement therapy and the patient's menstrual cycle to ensure the timing of the scan is optimal. Finally, a clear path is outlined for the completion and submission of the form, underscoring the importance of seamless communication between the referring physician’s office and the imaging center, all aimed at facilitating a safe, accurately diagnosed, and efficient patient care experience.
| Question | Answer |
|---|---|
| Form Name | Rutland Form 2772 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 183MRI_Order Prescreening_Qu estionnaire_277 2 mri fill in the blanks form |

Outpatient MRI Order/ Prescreening Questionnaire
Upon completion, please fax to central scheduling at
(For Breast MRI only, fax to Breast Care Program at
Patient Name: ____________________________________ |
Date of Birth: _______________________________ |
|
Patient Phone |
Referring Physician: _________________________ |
|
Can we leave a message? Yes No |
Physician Signature: ________________________ |
|
(If not, please have patient call us the next business day |
Date and Time: ____________________________ |
|
77002 Fluoroscopy for needle placement for MR arthrogram injection |
MR Arthrogram ___________ |
|
Type of MRI ordered: ________________________________ IV contrast with |
without with and without |
|
Diagnosis/What are we looking for? _______________________________________________________________
Symptomatology/Findings: ______________________________________________________________________
YES NO PLEASE ANSWER EACH QUESTION
Does patient have a pacemaker (or pacemaker wires in chest), implantable cardiovascular device (ICD) or external device (insulin pump)?
Does patient have a brain aneurysm clip? If yes, call MRI at
Does patient have fear of close places (claustrophobia)? If yes, physician to specify minimal |
|||
or moderate sedation? |
minimal (anxiolysis) |
moderate |
|
Is patient ≥ 60 years of age? |
Yes No |
Patient weight: __________ |
|
Is patient diabetic? Yes |
No |
Patient height: __________ |
|
If the patient is diabetic or over 60years of age a BUN and Creatinine is required (within 90 days) if patient is receiving contrast.
BUN_________ CREATININE_______ DATE________
Has patient ever had eye surgery that resulted in implants other than cataract lens?
If yes, what/when? ___________________________________________________________
Has patient ever had ear surgery that resulted in a metal cochlear implant? If yes, call MRI with type of implant. ___________________________________________
Has patient ever had an accident with metal in the eye? If yes, have they had an MRI since? If not, patient must have an
Has patient had any recent prior surgery, as MRIs should be done
Does patient have any implanted devices (other than cataract lenses)?
If yes, what? _______________________________________________________________
Is patient pregnant or think she may be pregnant? Yes No Is patient a nursing mother? Yes No
Does patient have difficulty lying flat on his/her back or stomach? If so, which?___________
ONLY FOR MRI OF BREAST:
Is patient on hormone replacement therapy (HRT)? If yes, patient needs to be off HRT for 6 weeks before MRI is performed. Date of last dose: ______________________
First day of last menstrual period: ____________ Date next period expected: ____________
MRI must be at least 6 months after end of radiation treatment; at least 1 year after end of chemotherapy.
Above portion completed by_____________________________ Date/Time _________________________
TO BE COMPLETED BY CENTRAL SCHEDULING:
MRUN: _____________ Booked by: _________ Date/Time: ________________ Confirmation #: __________
Other Exams: ___________________________________ MRI scheduled for:__________________________
FORM # 2772 REV. 03/08; 05/08, 09/08, 12/08, 5/09