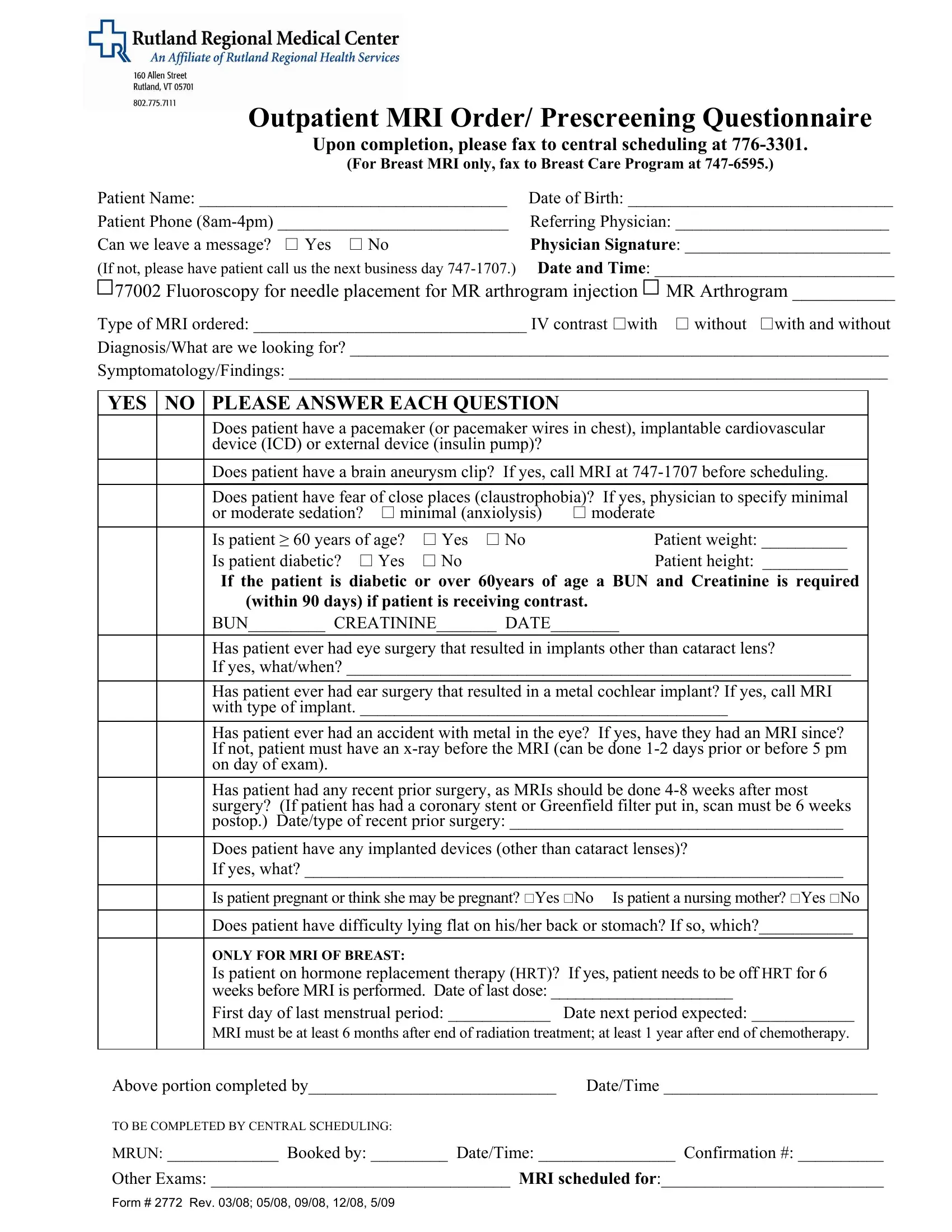
Ensuring a patient's safety and appropriate care during an MRI scan involves thorough preparation and screening. The Rutland 2772 form is a crucial document in this process, designed for outpatient MRI orders and prescreening questionnaires. Its use is a testament to the meticulous attention given to both medical and procedural aspects of MRI diagnostics. This form collects comprehensive patient information, including their name, date of birth, and contact details, ensuring clear identification and communication. Physicians are required to fill in specific details about the type of MRI ordered, highlighting whether IV contrast is needed and the diagnosis they are investigating. In addition to procedural details, the form meticulously screens for potential hazards or complications by inquiring about conditions like pacemakers, brain aneurysm clips, claustrophobia, and metal implants. Such precautions are vital, considering the strong magnetic fields used in MRI scans. The prescreening also considers the patient’s physical ability to undergo an MRI, asking about their ability to lie flat, and special considerations such as pregnancy or the patient being a nursing mother. For breast MRIs, the form inquires about hormone replacement therapy and the patient's menstrual cycle to ensure the timing of the scan is optimal. Finally, a clear path is outlined for the completion and submission of the form, underscoring the importance of seamless communication between the referring physician’s office and the imaging center, all aimed at facilitating a safe, accurately diagnosed, and efficient patient care experience.
| Question | Answer |
|---|---|
| Form Name | Rutland Form 2772 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 183MRI_Order Prescreening_Qu estionnaire_277 2 mri fill in the blanks form |
