


Our PDF editor makes it simple to complete documents. There's no need to do much to update la owca second injury questionnaire documents. Simply comply with these actions.
Step 1: Choose the "Get Form Here" button.
Step 2: Now, you can start modifying the louisiana questionnaire. The multifunctional toolbar is at your disposal - insert, eliminate, transform, highlight, and perform many other commands with the words and phrases in the form.
To fill out the file, type in the data the platform will ask you to for each of the appropriate sections:
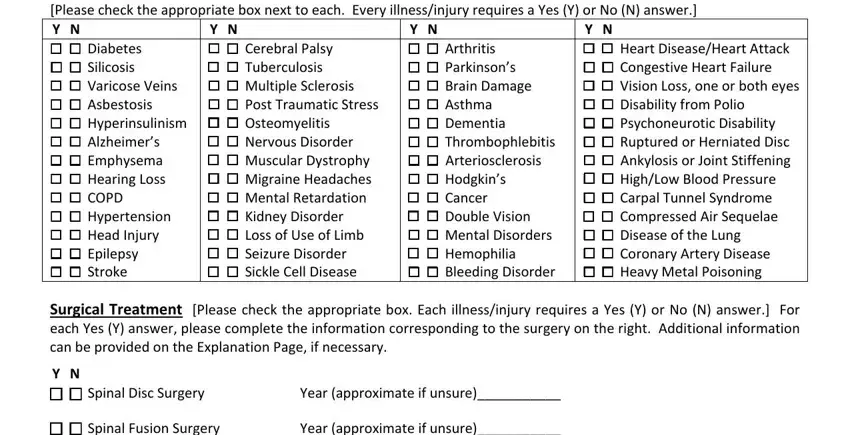
Fill in the Disease and Other Medical, Y N Cerebral Palsy, Y N Heart DiseaseHeart Attack, Y N Arthritis Parkinsons, Hodgkins Cancer Double, Surgical Treatment Please check, Y N Spinal Disc Surgery, Year approximate if unsure, Spinal Fusion Surgery, and Year approximate if unsure section with the details asked by the program.
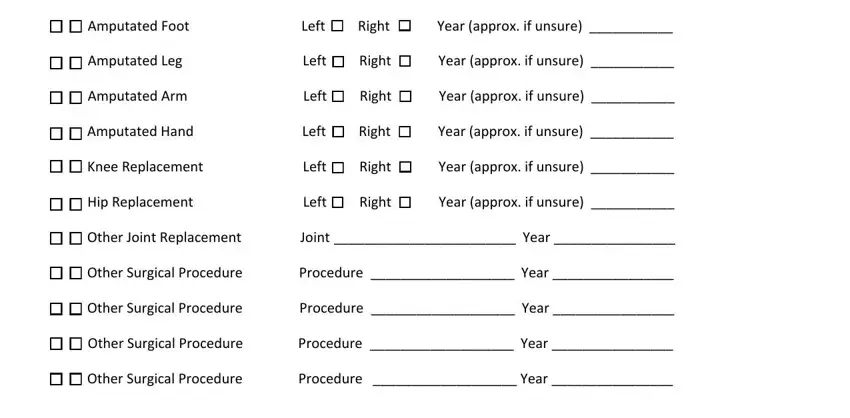
Put in writing any particulars you need within the area Spinal Fusion Surgery, Year approximate if unsure, Amputated Foot Left, Right, Year approx if unsure, Amputated Leg Left, Right, Year approx if unsure, Amputated Arm Left, Right, Year approx if unsure, Amputated Hand Left, Right, Year approx if unsure, and Knee Replacement.
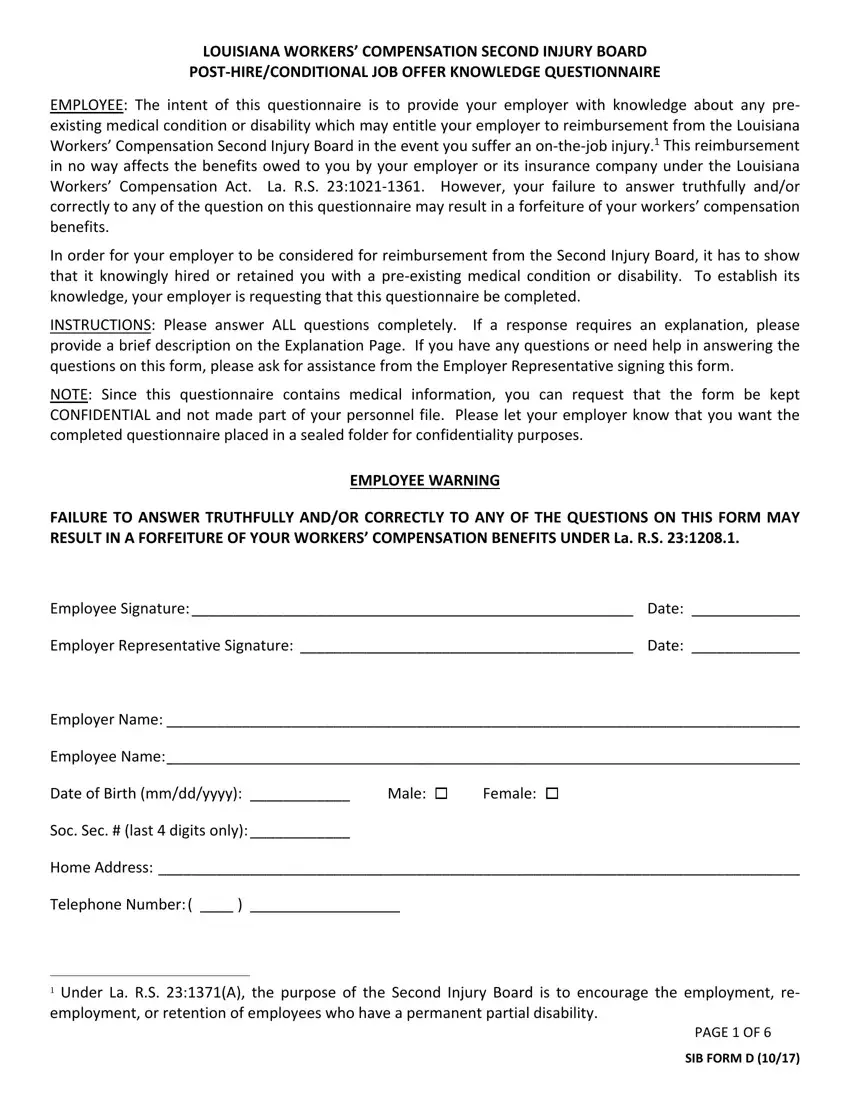
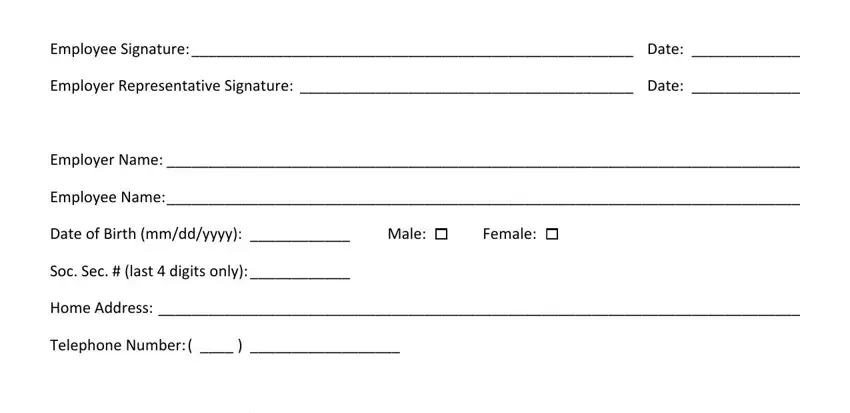
The Employee Signature, Date, Employer Representative, Date, PAGE OF, and SIB FORM D area will be used to note the rights or obligations of both sides.
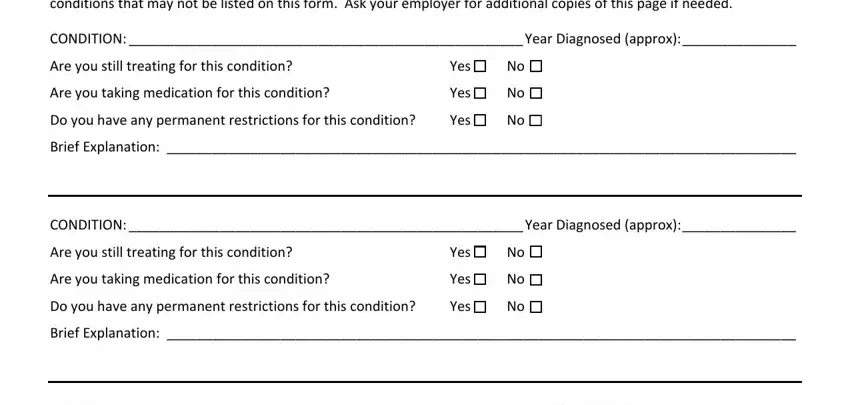
Finish by reading the following fields and completing them as required: EXPLANATION PAGE Please use the, CONDITION Year Diagnosed approx, Are you still treating for this, Are you taking medication for this, Yes, Yes, Do you have any permanent, Yes, Brief Explanation, CONDITION Year Diagnosed approx, Are you still treating for this, Are you taking medication for this, Yes, Yes, and Do you have any permanent.
Step 3: After you have hit the Done button, your document is going to be obtainable for upload to every device or email address you indicate.
Step 4: Produce copies of your form. This can save you from forthcoming complications. We don't watch or reveal your data, therefore feel comfortable knowing it will be safe.
