
Completing the worry questionnaire pdf form is not hard with our PDF editor. Keep up with these particular steps to prepare the document in no time.
Step 1: Press the orange "Get Form Now" button on the page.
Step 2: Now you can manage your worry questionnaire pdf. Feel free to use our multifunctional toolbar to add, delete, and alter the content material of the file.
The particular segments will help make up the PDF form:
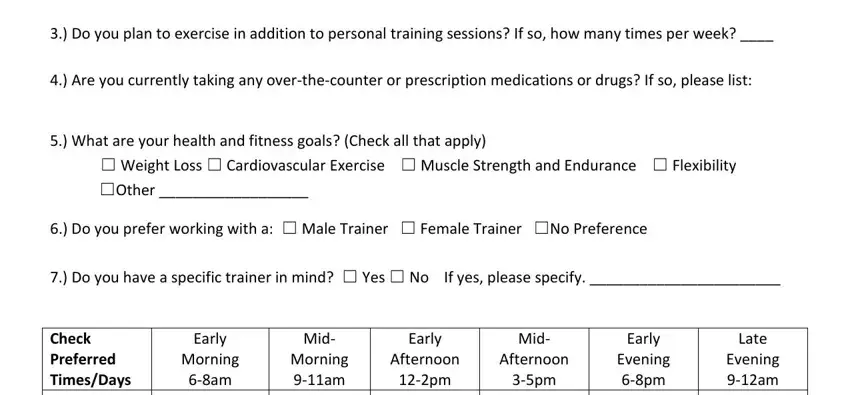
Remember to fill up the Do you plan to exercise in, Are you currently taking any, What are your health and fitness, Weight Loss Cardiovascular, Other, Do you prefer working with a, Do you have a specific trainer in, Early Morning am, Mid Morning am, Early Afternoon pm, Mid Afternoon pm, Early Evening pm, Late Evening am, and Check Preferred TimesDays MONDAY field with the appropriate information.
Identify the most vital details of the Check Preferred TimesDays MONDAY, and WEDNESDAY THURSDAY FRIDAY SATURDAY area.
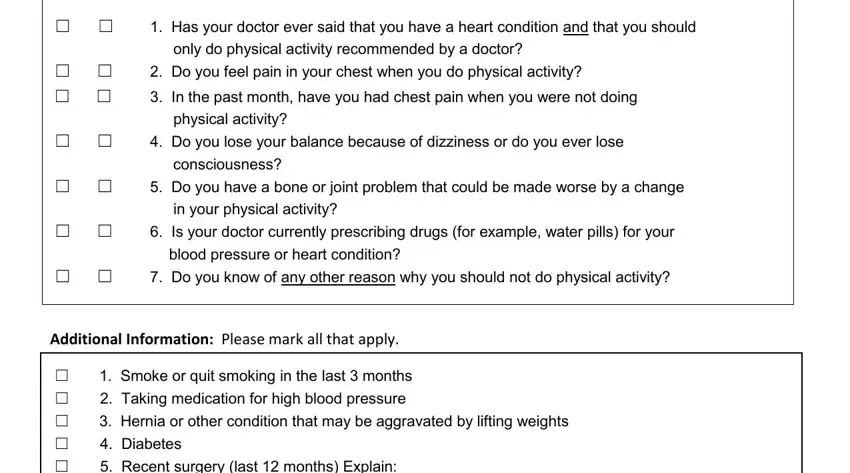
The Has your doctor ever said that, Do you feel pain in your chest, In the past month have you had, Do you lose your balance because, only do physical activity, Is your doctor currently, Do you know of any other reason, Do you have a bone or joint, Additional Information Please mark, Smoke or quit smoking in the, and Diabetes field is the place to put the rights and responsibilities of either side.
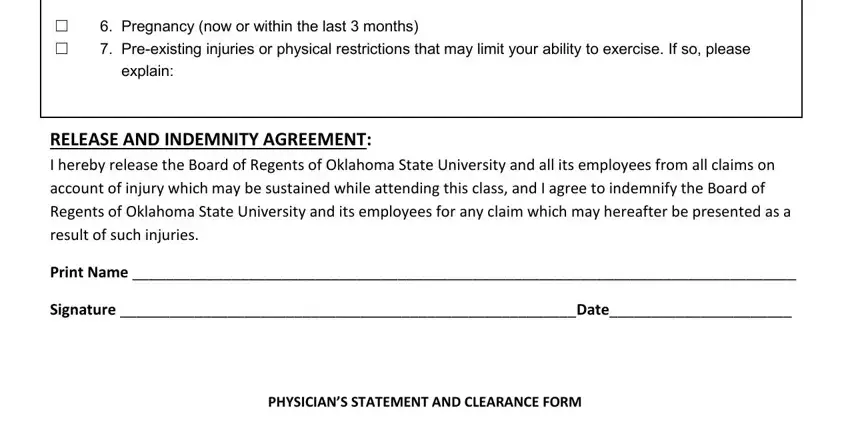
Look at the sections Pregnancy now or within the last, explain, RELEASE AND INDEMNITY AGREEMENT I, Print Name, Signature Date, and PHYSICIANS STATEMENT AND CLEARANCE and next complete them.
Step 3: As soon as you've clicked the Done button, your document is going to be readily available export to any type of electronic device or email address you identify.
Step 4: Just be sure to generate as many duplicates of the file as you can to prevent possible misunderstandings.
