

You can certainly obtain documents through our PDF editor. Improving the pearson vue cna license renewal file is easy should you try out these actions:
Step 1: You can hit the orange "Get Form Now" button at the top of this page.
Step 2: So, you're on the document editing page. You may add information, edit present information, highlight specific words or phrases, insert crosses or checks, add images, sign the template, erase unnecessary fields, etc.
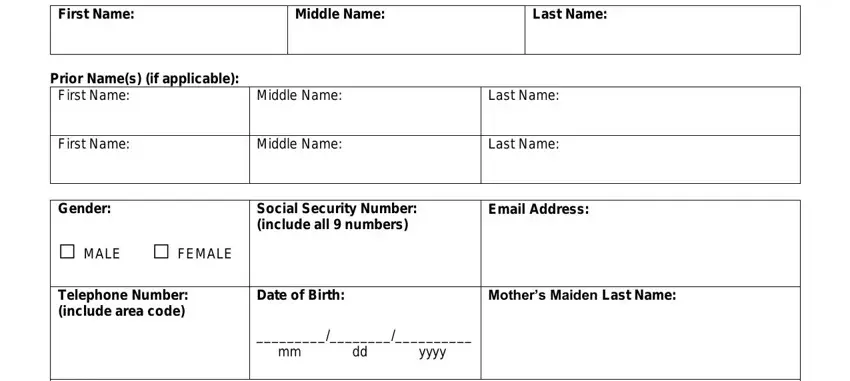
You should enter the following details to prepare the pearson vue cna license renewal PDF:
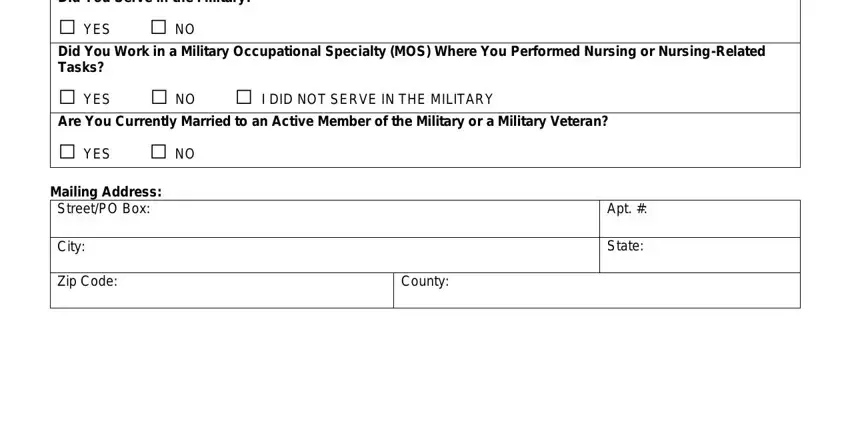
Feel free to complete the Did You Serve in the Military, YES NO, Did You Work in a Military, YES NO I DID NOT SERVE IN THE, Are You Currently Married to an, YES NO, Mailing Address StreetPO Box, City, Zip Code, Apt, State, and County box with the essential information.
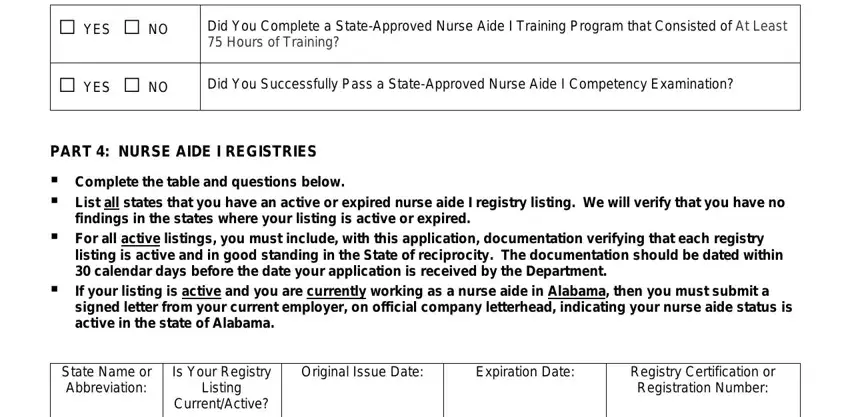
It is crucial to record certain details in the space YES NO, YES NO, Did You Complete a StateApproved, Did You Successfully Pass a, PART NURSE AIDE I REGISTRIES, Complete the table and questions, findings in the states where your, For all active listings you must, listing is active and in good, If your listing is active and you, signed letter from your current, State Name or Abbreviation, Is Your Registry Listing, Original Issue Date, and Expiration Date.
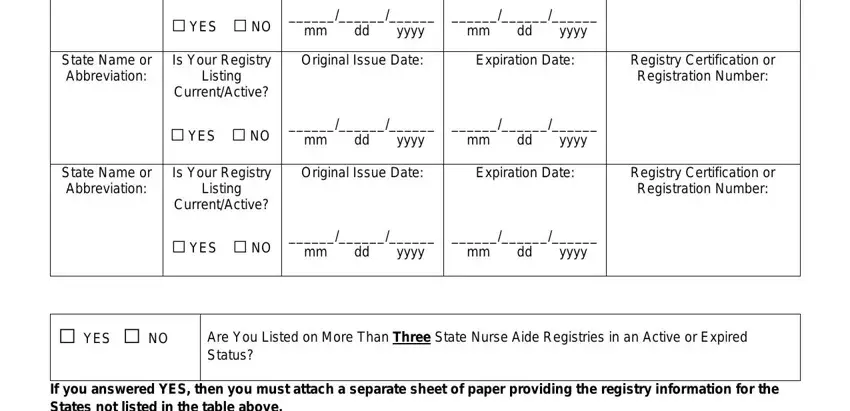
Inside of field YES NO, mm dd yyyy, mm dd yyyy, State Name or Abbreviation, Is Your Registry Listing, Original Issue Date, Expiration Date, Registry Certification or, YES NO, mm dd yyyy, mm dd yyyy, State Name or Abbreviation, Is Your Registry Listing, Original Issue Date, and Expiration Date, indicate the rights and responsibilities.
Finish the form by looking at these areas: YES NO, Do You Have Any Pending or, If you answered YES to the, States Where You Have a Pending or, PART EMPLOYMENT TYPE, Select the employment type where, Select all that apply, AdultFamily Care Home, Home HealthHome Care, Hospice, Hospital, Mental Health, Nursing Home, and Other please specify.
Step 3: Hit "Done". Now you can upload the PDF file.
Step 4: In order to prevent any specific challenges as time goes on, try to get a minimum of a few copies of the document.
