Our PDF editor was created to be as easy as possible. While you comply with the following steps, the procedure for filling in the new jerseysp 41 application document is going to be effortless.
Step 1: Choose the button "Get Form Here" on this site and press it.
Step 2: Now, you are on the document editing page. You can add content, edit existing data, highlight certain words or phrases, insert crosses or checks, add images, sign the file, erase unwanted fields, etc.
The PDF document you decide to fill out will cover the next parts:
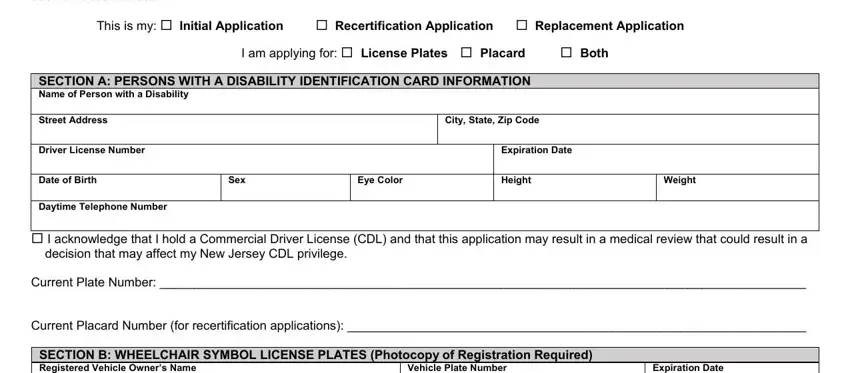
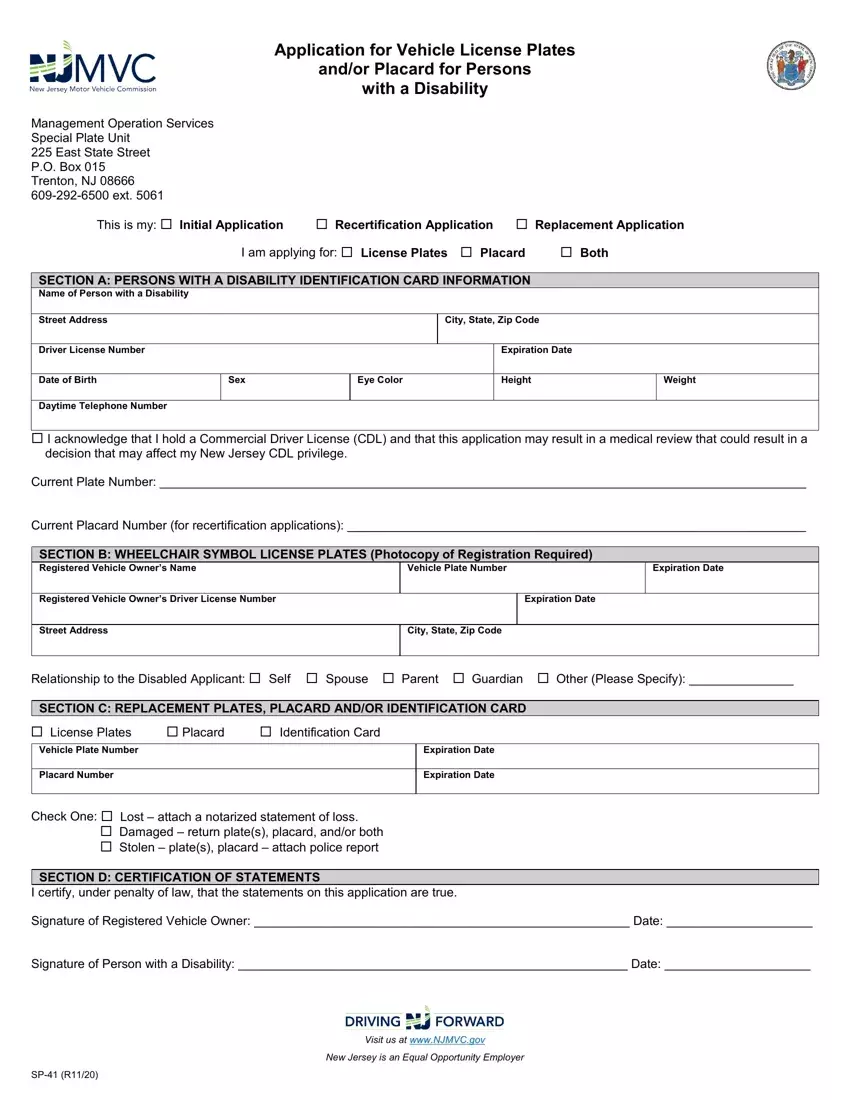
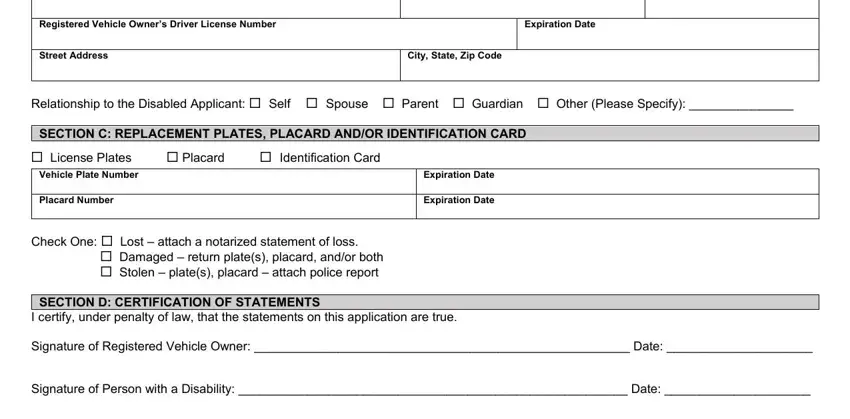
Write the necessary information in the SECTION B WHEELCHAIR SYMBOL, Vehicle Plate Number, Expiration Date, Registered Vehicle Owners Driver, Expiration Date, Street Address, City State Zip Code, Relationship to the Disabled, SECTION C REPLACEMENT PLATES, License Plates, Placard, Identification Card, Vehicle Plate Number, Placard Number, and Expiration Date area.
It is crucial to note particular details in the segment SP R, Visit us at wwwNJMVCgov, and New Jersey is an Equal Opportunity.

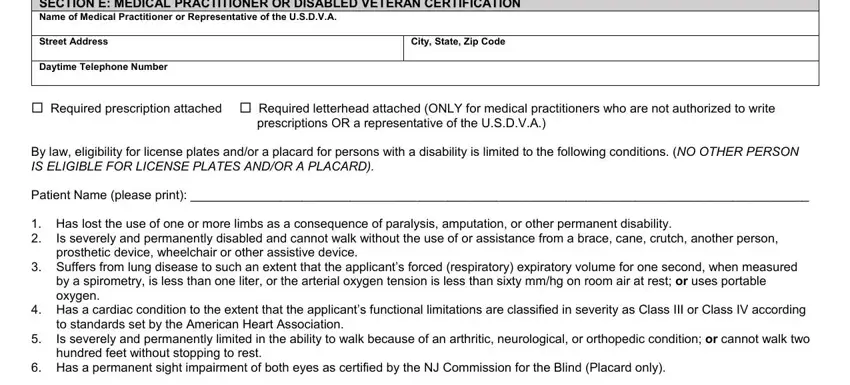
Please make sure to specify the rights and obligations of the parties inside the SECTION E MEDICAL PRACTITIONER OR, Street Address, Daytime Telephone Number, City State Zip Code, Required prescription attached, By law eligibility for license, Patient Name please print, Has lost the use of one or more, Is severely and permanently, Suffers from lung disease to such, Has a cardiac condition to the, to standards set by the American, and Has a permanent sight impairment paragraph.
Fill in the document by taking a look at the next sections: I CERTIFY UNDER PENALTY OF LAW, Signature of Medical Practitioner, SECTION F TERMS AND CONDITIONS, Pursuant of NJSA C a NJSA C and, Wheelchair symbol license plates, member providing transportation, Wheelchair symbol license plates, parking space and must be removed, Persons with a Disability, for license platesplacard as, The persons with a Disability, identification card The, and Application for a Persons with a.
Step 3: Press the Done button to confirm that your completed file is available to be exported to any gadget you pick out or mailed to an email you indicate.
Step 4: Create duplicates of the file - it can help you avoid forthcoming problems. And don't get worried - we are not meant to publish or check your data.
