
In case you wish to fill out Pedodontics, there's no need to download any kind of software - simply try using our online PDF editor. The tool is constantly upgraded by our team, acquiring awesome functions and turning out to be a lot more versatile. This is what you'd want to do to begin:
Step 1: Open the form in our tool by clicking on the "Get Form Button" above on this page.
Step 2: With the help of this advanced PDF editing tool, you could do more than simply fill in blanks. Express yourself and make your forms seem perfect with custom text added, or modify the original content to perfection - all backed up by an ability to insert your personal pictures and sign the file off.
This document requires specific data to be filled out, thus you need to take the time to fill in precisely what is requested:
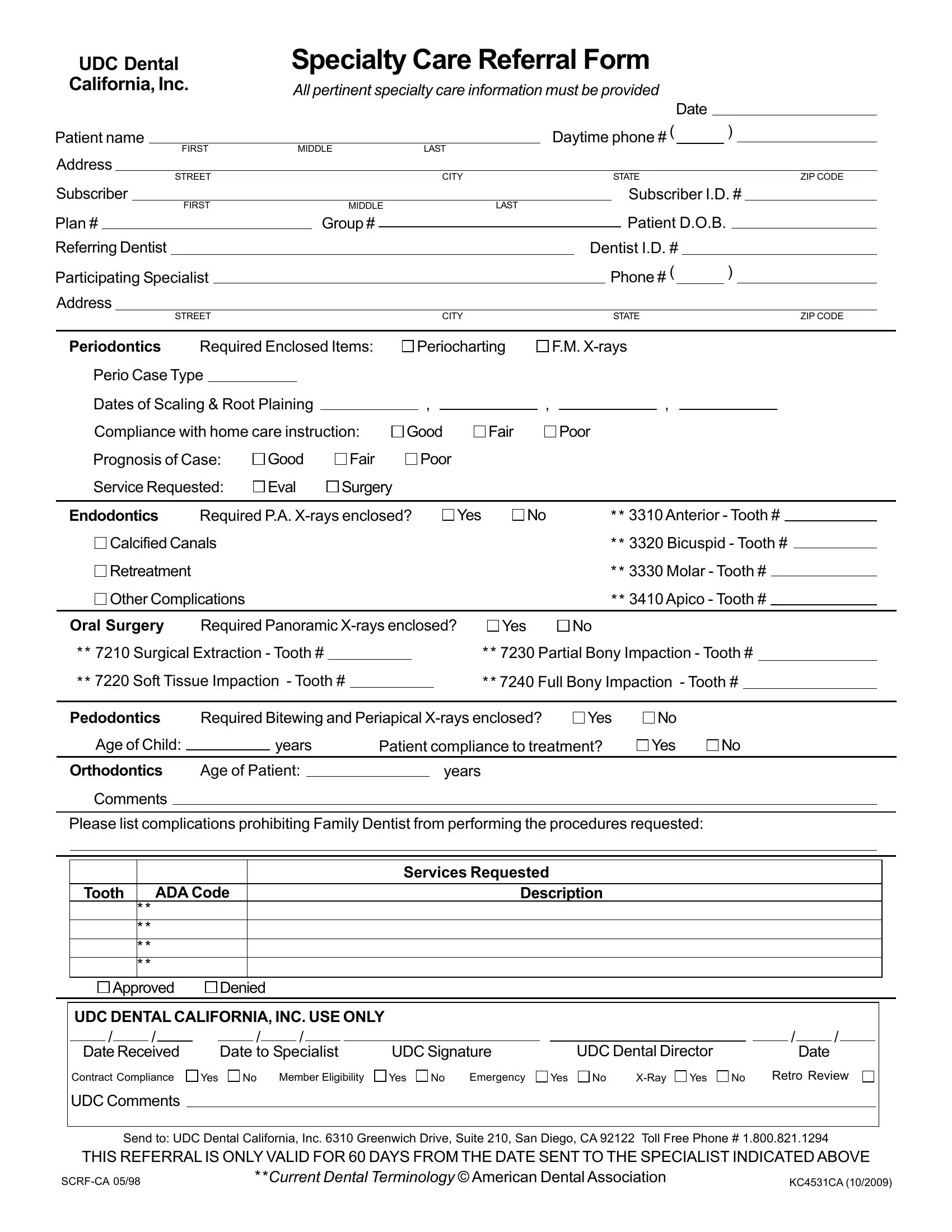
1. It's vital to fill out the Pedodontics accurately, thus be mindful while filling out the areas including all these blank fields:
2. Right after performing this section, head on to the subsequent stage and enter the essential details in all these fields - Retreatment, Other Complications, Molar Tooth, Apico Tooth, Oral Surgery, Required Panoramic Xrays enclosed, Yes, Surgical Extraction Tooth, Partial Bony Impaction Tooth, Soft Tissue Impaction Tooth, Full Bony Impaction Tooth, Pedodontics, Required Bitewing and Periapical, Yes, and Age of Child.
You can easily make errors when completing the Molar Tooth, so ensure that you take another look before you'll submit it.
Step 3: Before moving on, make sure that blanks have been filled out the right way. When you believe it's all fine, click “Done." Make a 7-day free trial plan at FormsPal and get immediate access to Pedodontics - downloadable, emailable, and editable inside your FormsPal cabinet. FormsPal is devoted to the confidentiality of all our users; we make sure that all information coming through our editor is confidential.