
Once you open the online editor for PDFs by FormsPal, you can complete or change ssa form 4641 here and now. To make our editor better and less complicated to utilize, we consistently implement new features, considering feedback coming from our users. For anyone who is seeking to get going, here's what it will require:
Step 1: Hit the "Get Form" button above. It will open our editor so that you could begin filling in your form.
Step 2: This tool provides you with the opportunity to work with PDF files in many different ways. Transform it with your own text, correct original content, and place in a signature - all manageable in no time!
It is actually straightforward to finish the form with this practical guide! Here is what you want to do:
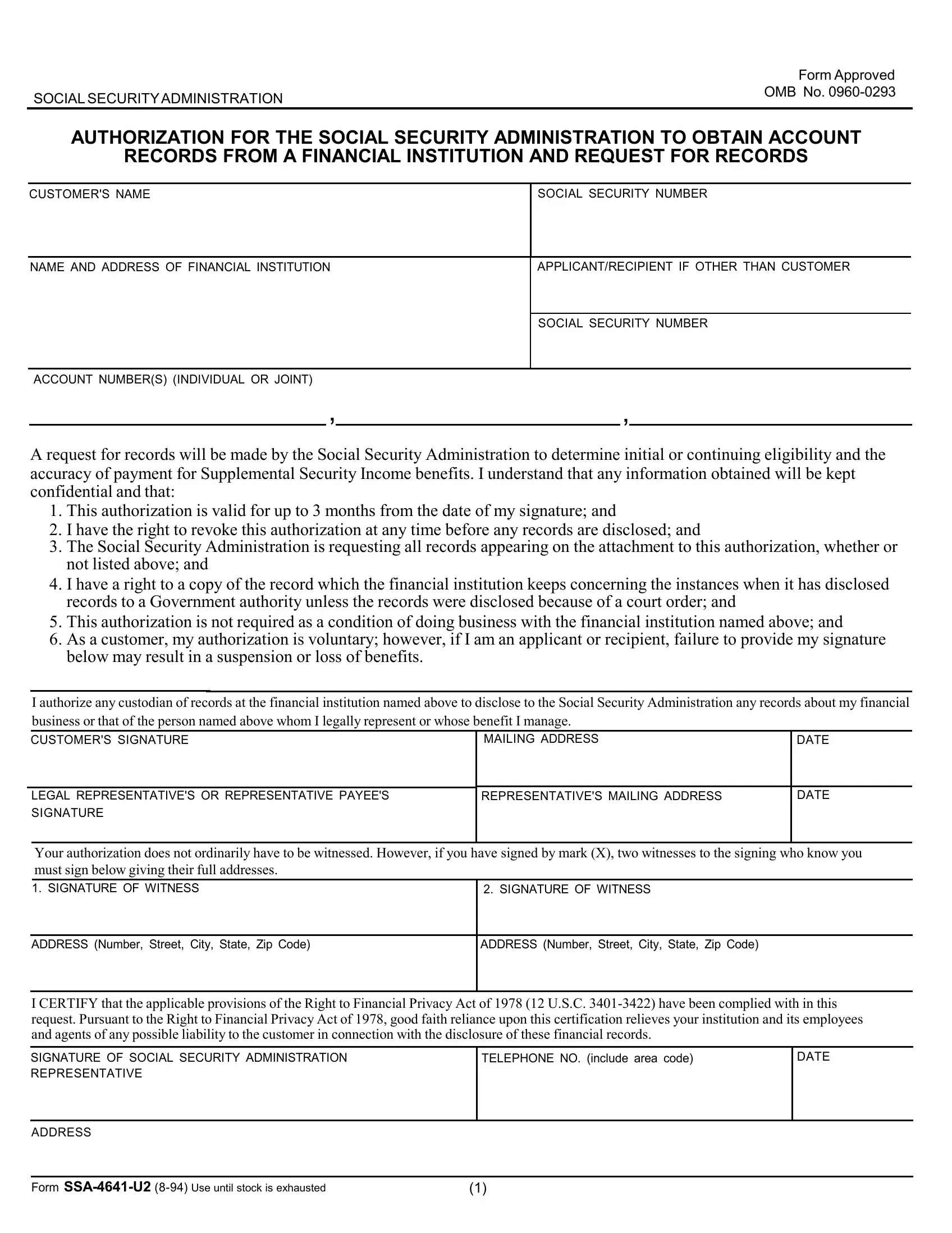
1. It's very important to complete the ssa form 4641 accurately, thus be careful while filling in the sections containing these particular blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - I authorize any custodian of, CUSTOMERS SIGNATURE, MAILING ADDRESS, DATE, LEGAL REPRESENTATIVES OR, REPRESENTATIVES MAILING ADDRESS, DATE, Your authorization does not, SIGNATURE OF WITNESS, ADDRESS Number Street City State, ADDRESS Number Street City State, I CERTIFY that the applicable, SIGNATURE OF SOCIAL SECURITY, TELEPHONE NO include area code, and DATE with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
Always be very attentive while filling in DATE and MAILING ADDRESS, as this is the section where most people make a few mistakes.
3. This next segment will be about ADDRESS, and Form SSAU Use until stock is - fill out all these blank fields.

4. You're ready to fill in this next form section! In this case you've got these PLEASE BE SURE TO SIGN AND DATE, ADDITIONAL INFORMATIONREMARKS FROM, and Form SSAU empty form fields to complete.
5. This document should be finished by filling in this segment. Below there is a detailed listing of blank fields that require correct information for your form submission to be complete: Customers Name, Customers Social Security Number, Financial Institution Name and, ApplicantRecipient If Not Customer, Social Security Number, Account Numberss Individual or, The financial institution is, PART IIFOR COMPLETION BY THE, This request is authorized by, and INSTRUCTIONS FOR COMPLETION cid cid.
Step 3: Before moving on, make certain that all blank fields were filled out right. As soon as you are satisfied with it, click on “Done." Go for a 7-day free trial subscription at FormsPal and obtain immediate access to ssa form 4641 - which you'll be able to then work with as you wish from your FormsPal cabinet. When you work with FormsPal, it is simple to fill out forms without stressing about database breaches or data entries getting shared. Our secure system ensures that your personal details are stored safe.