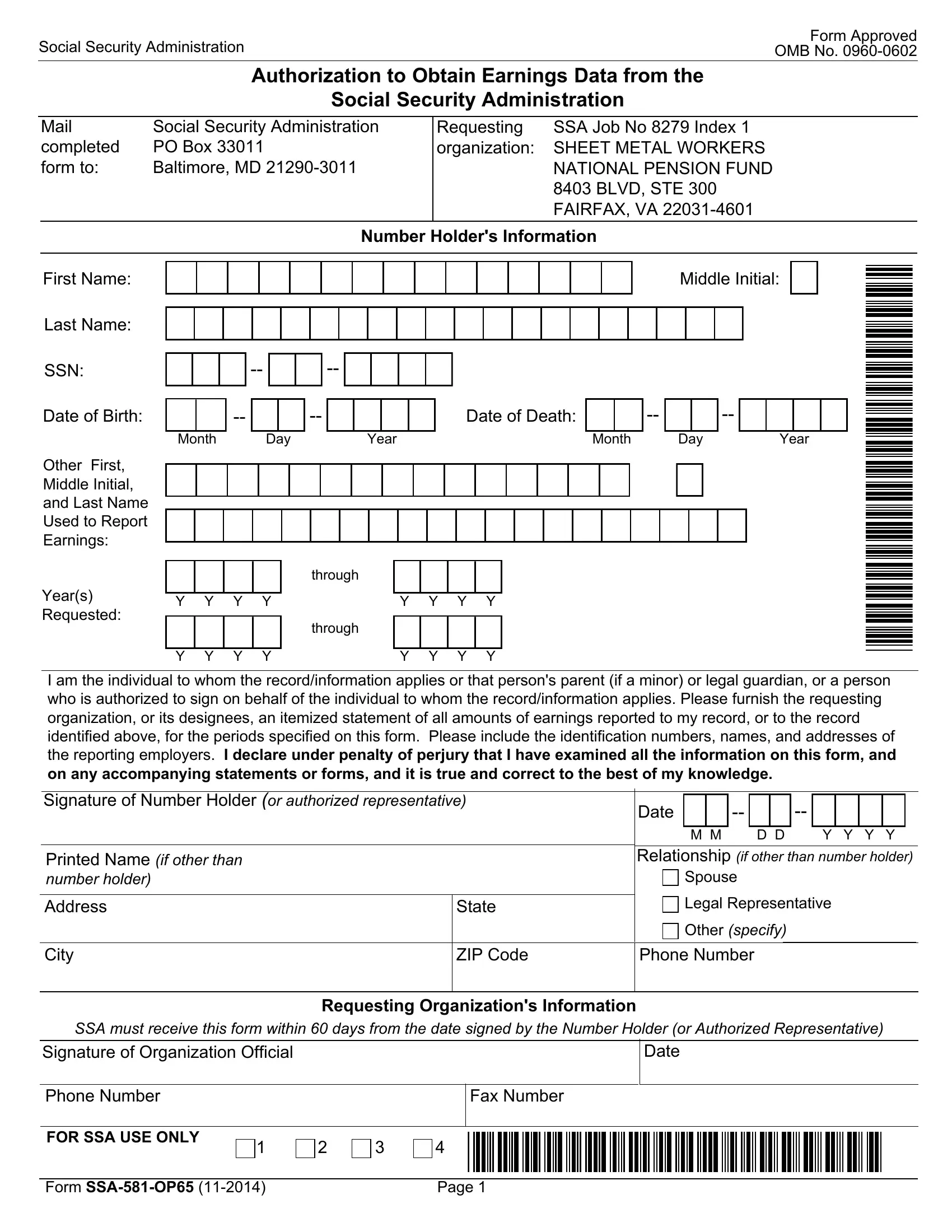
The Social Security Administration (SSA) has a form known as SSA-581-OP65, a crucial document for individuals or organizations needing to obtain earnings data from the SSA. This form serves as an authorization for the Social Security Administration to release an itemized statement of earnings reported to an individual's social security record for specified years. Designed to facilitate a range of requests, including but not limited to personal record keeping, legal proceedings, or pension fund management, this form is necessary for the Sheet Metal Workers National Pension Fund, highlighted as the requesting organization in the given example. Located in Fairfax, VA, this organization, like many others, relies on accurate earnings data for its operations. Applicants must fill in personal details, including Social Security Number (SSN), and specify the years for which earnings data is requested. Importantly, the form comes with a declaration under penalty of perjury, underscoring the serious legal obligation of the applicant to provide truthful information. Moreover, the SSA provides a Privacy Act Statement and a notice on the use of personal information, reassuring applicants about the confidentiality and restricted use of the data provided. The form also underscores the voluntary nature of providing information, while also hinting at potential implications of failing to supply the required data, which might affect the timely and accurate processing of claims. This document emphasizes the administration's commitment to privacy and the efficient handling of personal earnings data, as well as the legal framework that applicants engage with when submitting this form. The deadline for submitting the form to the SSA, outlined to be within 60 days from the date of signing, ensures a measure of timeliness and urgency in the processing of such requests.
| Question | Answer |
|---|---|
| Form Name | Form Ssa 581 Op65 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | authorizes, ssa 581 op 59, STE, SSN |