

































































































 Continued on Page 4
Continued on Page 4
It shouldn’t be challenging to obtain ssa 4734 f4 sup pdf through our PDF editor. This is the way you will be able effortlessly develop your form.
Step 1: Initially, choose the orange "Get form now" button.
Step 2: The document editing page is currently available. Include information or modify current data.
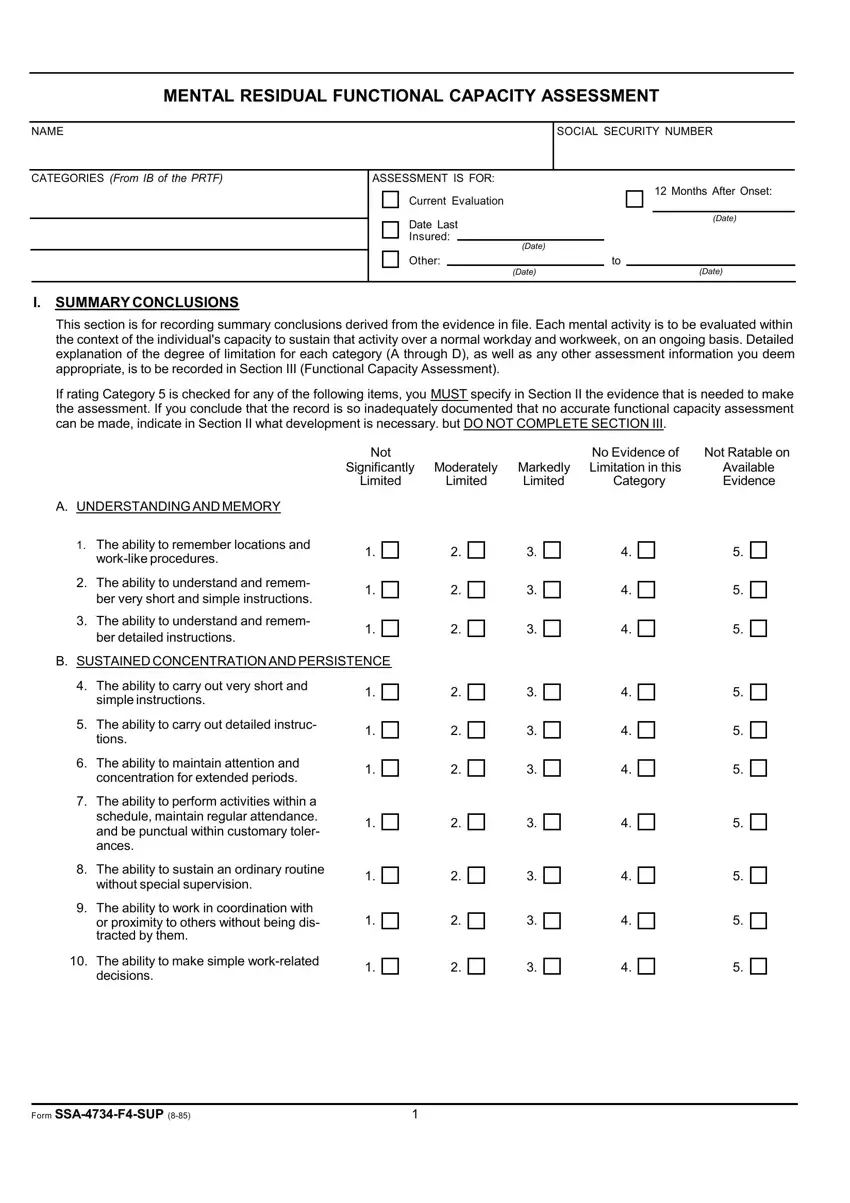
Prepare the ssa 4734 f4 sup pdf PDF and enter the information for each part:
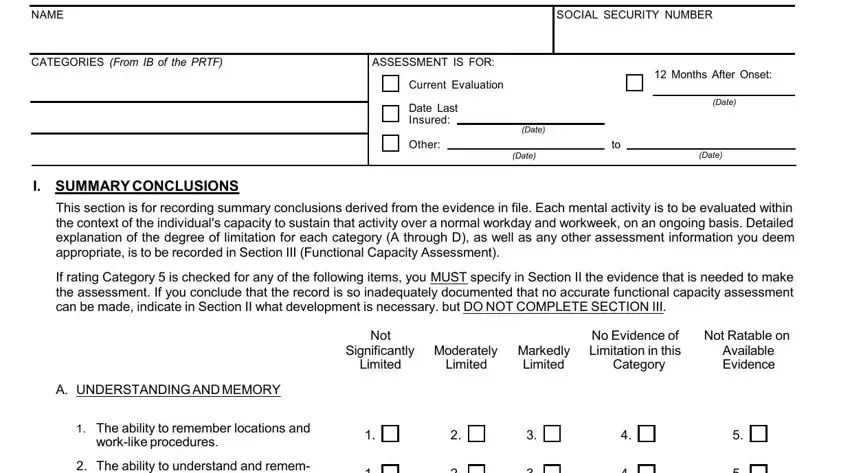
Enter the appropriate particulars in The ability to understand and, The ability to understand and, SUSTAINED CONCENTRATION AND, The ability to carry out very, The ability to carry out detailed, The ability to maintain attention, The ability to perform activities, The ability to sustain an ordinary, The ability to work in, and The ability to make simple section.
You're going to be required some fundamental details so that you can fill in the The ability to complete a normal, C SOCIAL INTERACTION, The ability to interact, The ability to ask simple, The ability to accept instructions, The ability to get along with, The ability to maintain socially, D ADAPTATION, The ability to respond, and The ability to be aware of normal section.
The space The ability to be aware of normal, The ability to travel in, The ability to set realistic goals, and REMARKS If you checked box for is where you insert both sides' rights and obligations.
Finish by reviewing these fields and completing them accordingly: Form SSAFSUP, and Continued on Page.

Step 3: When you have hit the Done button, your file is going to be ready for upload to each device or email you identify.
Step 4: Attempt to make as many duplicates of your form as you can to avoid potential problems.
