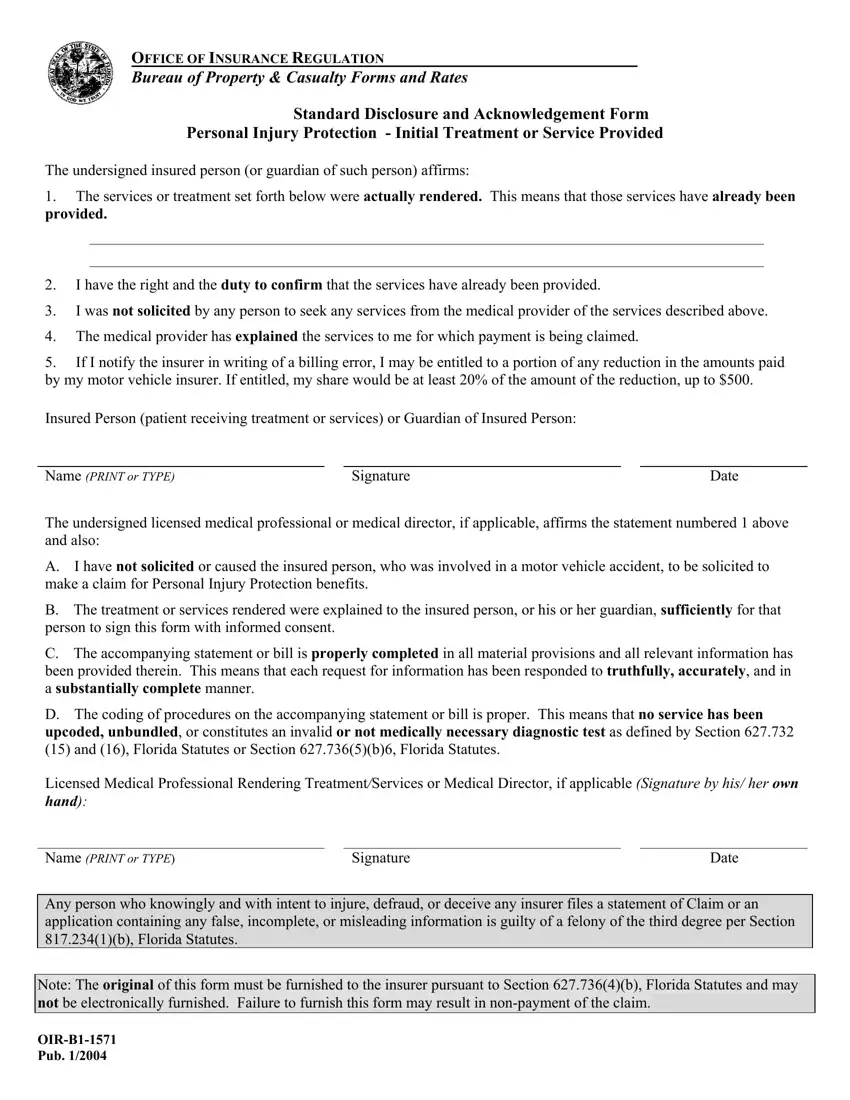
OFFICE OF INSURANCE REGULATION
Bureau of Property & Casualty Forms and Rates
Standard Disclosure and Acknowledgement Form
Personal Injury Protection - Initial Treatment or Service Provided
The undersigned insured person (or guardian of such person) affirms:
1.The services or treatment set forth below were actually rendered. This means that those services have already been provided.
2.I have the right and the duty to confirm that the services have already been provided.
3.I was not solicited by any person to seek any services from the medical provider of the services described above.
4.The medical provider has explained the services to me for which payment is being claimed.
5.If I notify the insurer in writing of a billing error, I may be entitled to a portion of any reduction in the amounts paid by my motor vehicle insurer. If entitled, my share would be at least 20% of the amount of the reduction, up to $500.
Insured Person (patient receiving treatment or services) or Guardian of Insured Person:
Name (PRINT or TYPE) |
Signature |
Date |
The undersigned licensed medical professional or medical director, if applicable, affirms the statement numbered 1 above and also:
A.I have not solicited or caused the insured person, who was involved in a motor vehicle accident, to be solicited to make a claim for Personal Injury Protection benefits.
B.The treatment or services rendered were explained to the insured person, or his or her guardian, sufficiently for that person to sign this form with informed consent.
C.The accompanying statement or bill is properly completed in all material provisions and all relevant information has been provided therein. This means that each request for information has been responded to truthfully, accurately, and in a substantially complete manner.
D.The coding of procedures on the accompanying statement or bill is proper. This means that no service has been
upcoded, unbundled, or constitutes an invalid or not medically necessary diagnostic test as defined by Section 627.732 (15) and (16), Florida Statutes or Section 627.736(5)(b)6, Florida Statutes.
Licensed Medical Professional Rendering Treatment/Services or Medical Director, if applicable (Signature by his/ her own hand):
Name (PRINT or TYPE) |
Signature |
Date |
Any person who knowingly and with intent to injure, defraud, or deceive any insurer files a statement of Claim or an application containing any false, incomplete, or misleading information is guilty of a felony of the third degree per Section 817.234(1)(b), Florida Statutes.
Note: The original of this form must be furnished to the insurer pursuant to Section 627.736(4)(b), Florida Statutes and may not be electronically furnished. Failure to furnish this form may result in non-payment of the claim.
OIR-B1-1571
Pub. 1/2004