


16th can be filled out online easily. Just use FormsPal PDF tool to do the job without delay. Our editor is consistently developing to provide the best user experience attainable, and that is because of our resolve for constant enhancement and listening closely to comments from users. By taking some basic steps, you'll be able to start your PDF journey:
Step 1: First, open the editor by pressing the "Get Form Button" above on this page.
Step 2: With our handy PDF file editor, it's possible to do more than simply fill out blank form fields. Express yourself and make your docs seem perfect with customized textual content added, or tweak the file's original input to excellence - all backed up by the capability to insert your personal photos and sign it off.
It is actually simple to finish the pdf using this detailed guide! This is what you should do:
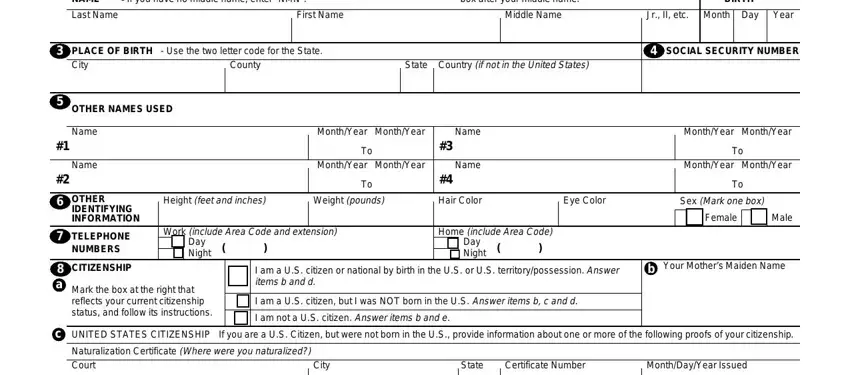
1. It is crucial to fill out the 16th accurately, so pay close attention while working with the areas containing all these blank fields:
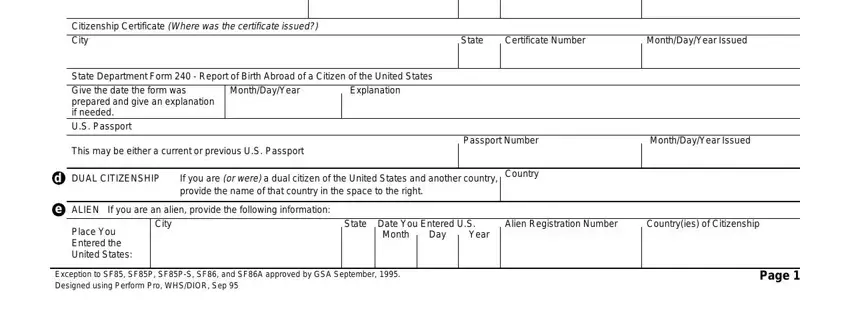
2. The third step would be to fill in the following fields: Citizenship Certificate Where was, State, Certificate Number, MonthDayYear Issued, State Department Form Report of, MonthDayYear, Explanation, This may be either a current or, Passport Number, MonthDayYear Issued, DUAL CITIZENSHIP, If you are or were a dual citizen, Country, ALIEN If you are an alien provide, and City.
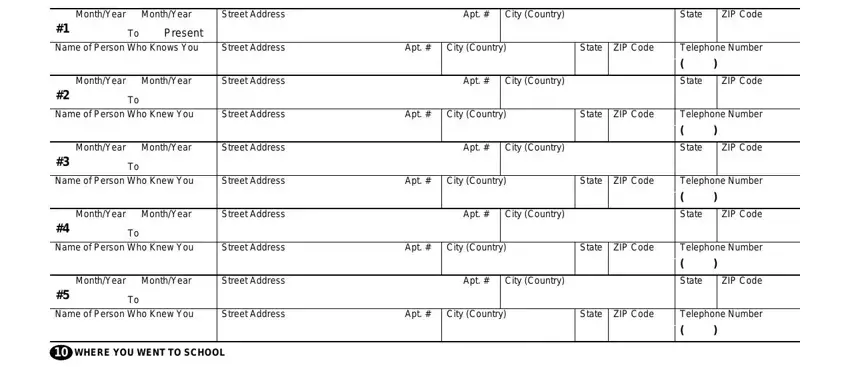
3. This next segment is all about MonthYear MonthYear, Street Address, Apt, City Country, State, ZIP Code, Present Name of Person Who Knows, Street Address, Apt, City Country, State ZIP Code, MonthYear MonthYear, Street Address, Apt, and City Country - fill out each one of these blank fields.
4. This next section requires some additional information. Ensure you complete all the necessary fields - For correspondence schools and, Name of School, Code, DegreeDiplomaOther, Street Address and City Country, MonthYear Awarded, State, ZIP Code, Name of Person Who Knew You, Street Address, Apt, City Country, State ZIP Code, MonthYear MonthYear, and Code - to proceed further in your process!
Be really careful when filling out Street Address and MonthYear Awarded, because this is where many people make a few mistakes.
5. The pdf should be completed by filling in this segment. Here you will see a comprehensive listing of form fields that require correct details in order for your document usage to be accomplished: Previous Periods of Activity, MonthYear MonthYear, Code, EmployerVerifier NameMilitary Duty, Your Position TitleMilitary Rank, Present EmployersVerifiers Street, City Country, State, ZIP Code, Street Address of Job Location if, City Country, State, ZIP Code, Supervisors Name Street Address, and City Country.
Step 3: Reread what you've typed into the blank fields and then click the "Done" button. Get hold of the 16th when you join for a 7-day free trial. Readily use the pdf file from your FormsPal account, together with any modifications and adjustments conveniently saved! When using FormsPal, you're able to fill out documents without needing to be concerned about personal information incidents or entries getting distributed. Our secure system makes sure that your personal data is maintained safely.