

Should you would like to fill out the std 610 form, you don't need to download and install any sort of applications - simply make use of our PDF tool. To make our tool better and more convenient to use, we continuously develop new features, considering feedback from our users. This is what you would need to do to start:
Step 1: Open the PDF file inside our tool by pressing the "Get Form Button" in the top section of this page.
Step 2: With the help of our online PDF file editor, it is possible to accomplish more than merely complete blanks. Try all of the features and make your docs look faultless with custom text incorporated, or optimize the file's original input to excellence - all that backed up by the capability to insert any graphics and sign the PDF off.
As for the blanks of this particular PDF, here is what you need to know:
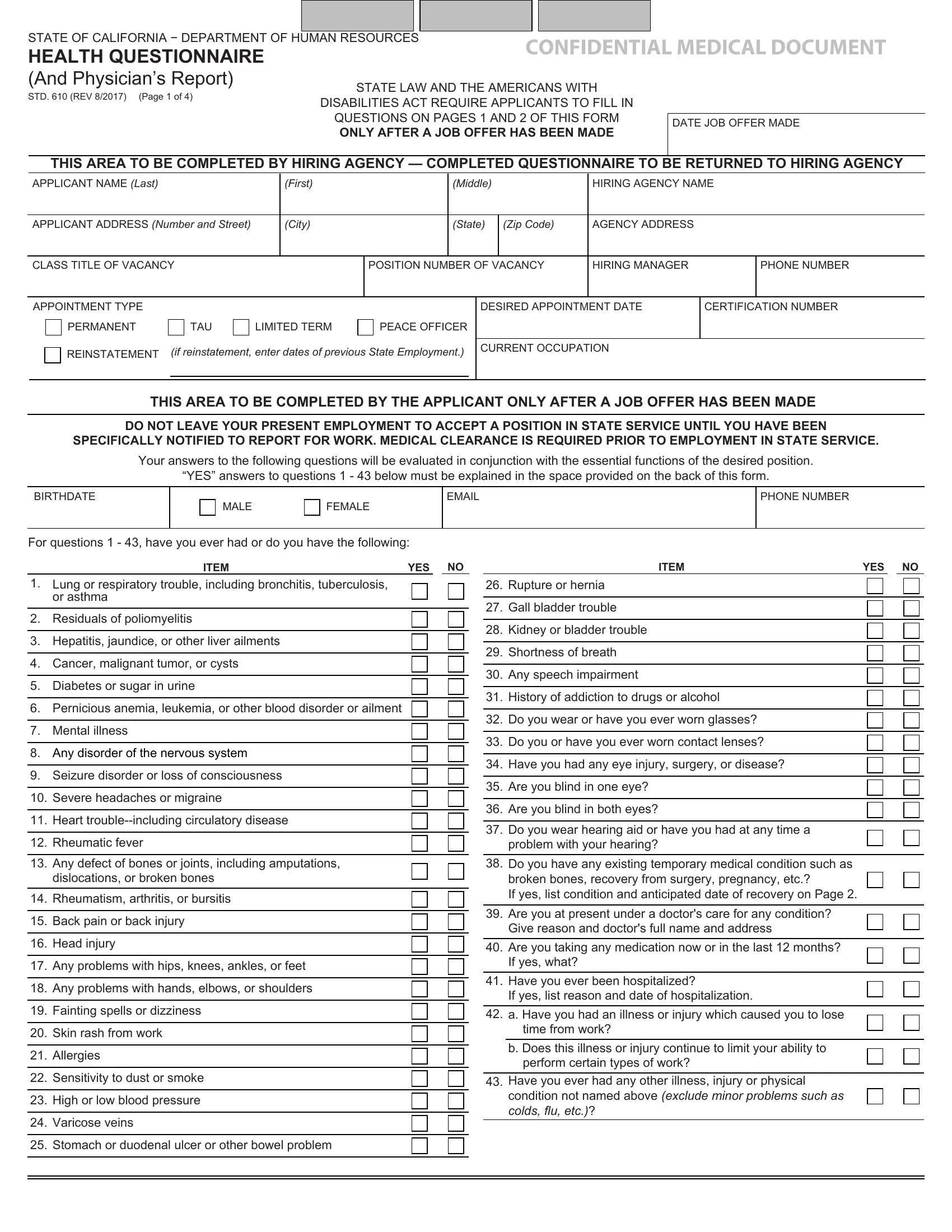
1. When filling out the the std 610 form, be sure to incorporate all necessary blank fields in the relevant section. It will help facilitate the work, which allows your information to be processed efficiently and accurately.
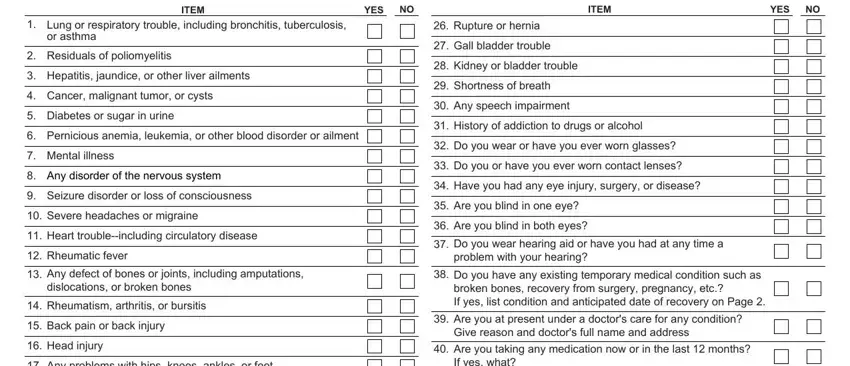
2. Once this array of fields is done, you need to insert the needed details in ITEM, YES, ITEM, YES, Lung or respiratory trouble, Residuals of poliomyelitis, Hepatitis jaundice or other liver, Cancer malignant tumor or cysts, Diabetes or sugar in urine, Pernicious anemia leukemia or, Mental illness, Any disorder of the nervous system, Seizure disorder or loss of, Severe headaches or migraine, and Heart troubleincluding circulatory in order to progress further.
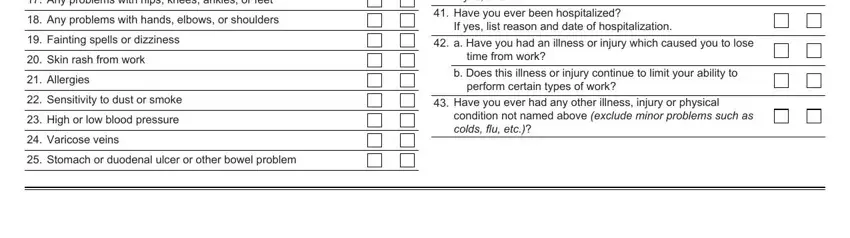
3. This next part is related to Any problems with hips knees, Any problems with hands elbows or, Fainting spells or dizziness, Skin rash from work, Allergies, Sensitivity to dust or smoke, High or low blood pressure, Varicose veins, Stomach or duodenal ulcer or other, Are you taking any medication now, Have you ever been hospitalized If, a Have you had an illness or, time from work, b Does this illness or injury, and perform certain types of work - type in each of these empty form fields.
4. Your next section will require your information in the following areas: APPLICANT NAME Last, First, Middle, HIRING AGENCY NAME, Please write your own account and, Include DATE OF ONSET YOUR PRESENT, Item, Explanation of YES Items, and Healthcare Provider and Contact. Ensure you provide all requested details to move further.
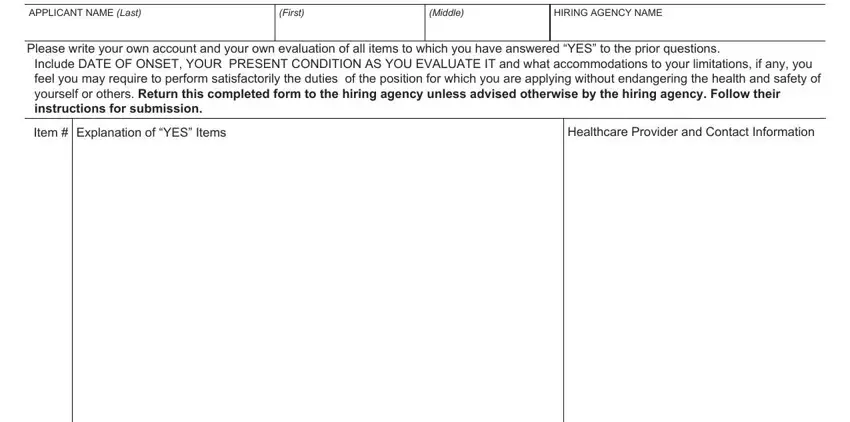
People who use this form often get some things wrong when filling out Healthcare Provider and Contact in this part. You should definitely revise what you type in here.
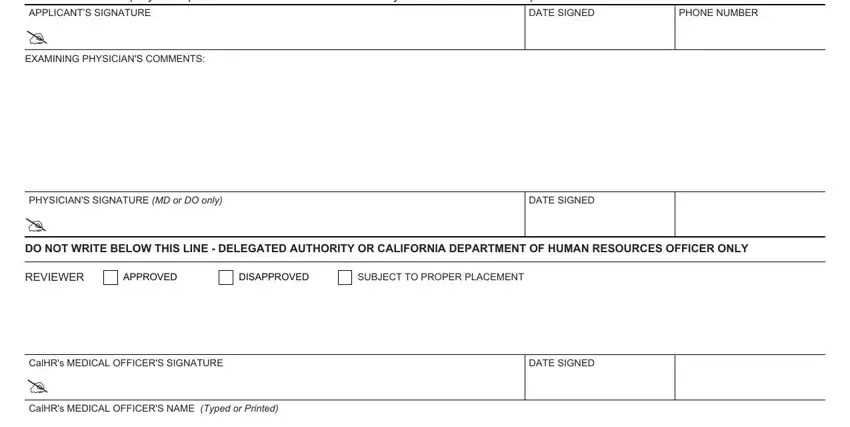
5. To finish your form, the particular area features several extra blank fields. Filling in CERTIFICATION I certify that I, APPLICANTS SIGNATURE, EXAMINING PHYSICIANS COMMENTS, DATE SIGNED, PHONE NUMBER, PHYSICIANS SIGNATURE MD or DO only, DATE SIGNED, DO NOT WRITE BELOW THIS LINE, REVIEWER, APPROVED, DISAPPROVED, SUBJECT TO PROPER PLACEMENT, CalHRs MEDICAL OFFICERS SIGNATURE, DATE SIGNED, and CalHRs MEDICAL OFFICERS NAME Typed will certainly wrap up the process and you can be done very fast!
Step 3: After going through your filled out blanks, click "Done" and you are good to go! Sign up with FormsPal now and immediately get the std 610 form, prepared for download. Each and every edit made is handily preserved , enabling you to modify the form at a later point if needed. Here at FormsPal, we aim to make certain that all of your details are maintained private.