The Special Transportation Service (STS) Application Form serves as a comprehensive document designed to evaluate and determine the eligibility of individuals for paratransit services in accordance with the Americans with Disabilities Act (ADA) of 1990. This pivotal form is divided into several sections, each capturing critical information about the applicant, starting from personal identification details such as Social Security number, date of birth, contact information, and residency, to more specific data concerning the applicant’s mobility aids, weight, and ability to transfer from a wheelchair to a vehicle with minimal assistance. Emergency contact details and voluntary disclosure of ethnicity for statistical purposes are also part of the applicant section. An essential aspect of the form is the applicant's release and consent, which emphasizes the confidential handling of sensitive information, the need for honesty in provided data, and the implications of submitting false information. Furthermore, the third section requires medical verification by a licensed physician in Florida, who must assess the applicant's disability through various categories and stipulate whether the disability impedes the use of public transportation services. The physician's input extends to indicating the type and nature of the individual's disabilities, the level of impairment, and the specific limitations that prevent the use of standard metro services. This detailed evaluation includes recommendations for the necessary mode of transportation and whether the presence of a personal care attendant is advisable for each trip. Additionally, the requirement for supporting medical documentation underscores the thoroughness of this process, aiming to ensure that eligible applicants receive the appropriate support tailored to their needs, while also safeguarding against misuse of the service.
| Question | Answer |
|---|---|
| Form Name | STS Application Form |
| Form Length | 7 pages |
| Fillable? | Yes |
| Fillable fields | 52 |
| Avg. time to fill out | 12 min 9 sec |
| Other names | special transportation services application, sts form 2021, how to fill sts form, sts form |
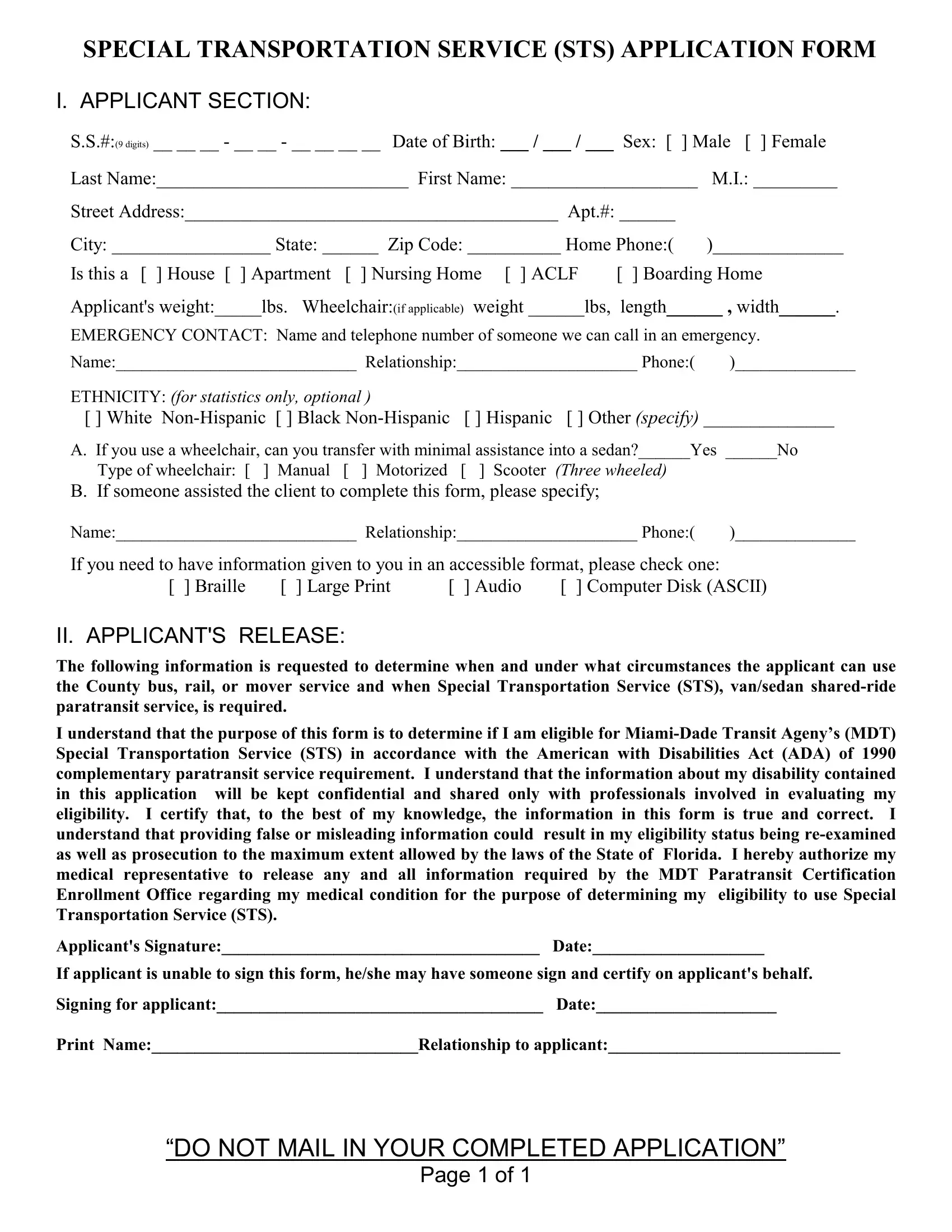
SPECIAL TRANSPORTATION SERVICE (STS) APPLICATION FORM
I. APPLICANT SECTION:
S.S.#:(9 digits) __ __ __ - __ __ - __ __ __ __ Date of Birth: ___ / ___ / ___ Sex: [ ] Male [ ] Female
Last Name:___________________________ First Name: ____________________ |
M.I.: _________ |
||||||
Street Address:________________________________________ Apt.#: ______ |
|
||||||
City: _________________ State: ______ Zip Code: __________ Home Phone:( |
)______________ |
||||||
Is this a [ ] House [ ] Apartment |
[ ] Nursing Home |
[ ] ACLF |
[ ] Boarding Home |
||||
Applicant's weight:_____lbs. Wheelchair:(if applicable) weight ______lbs, |
length______ , width______. |
||||||
EMERGENCY CONTACT: Name and telephone number of someone we can call in an emergency. |
|||||||
Name:____________________________ Relationship:_____________________ Phone:( |
)______________ |
||||||
ETHNICITY: (for statistics only, optional ) |
|
|
|
|
|
||
[ ] White |
[ ] Other (specify) ______________ |
||||||
A. If you use a wheelchair, can you transfer with minimal assistance into a sedan?______Yes ______No |
|||||||
Type of wheelchair: [ |
] Manual |
[ ] Motorized |
[ ] |
Scooter |
(Three wheeled) |
|
|
B. If someone assisted the client to complete this form, please specify; |
|
|
|||||
Name:____________________________ Relationship:_____________________ Phone:( |
)______________ |
||||||
If you need to have information given to you in an accessible format, please check one: |
|||||||
[ ] Braille |
[ ] Large Print |
[ ] Audio |
[ ] Computer Disk (ASCII) |
||||
II. APPLICANT'S RELEASE:
The following information is requested to determine when and under what circumstances the applicant can use the County bus, rail, or mover service and when Special Transportation Service (STS), van/sedan
I understand that the purpose of this form is to determine if I am eligible for
Applicant's Signature:_____________________________________ Date:____________________
If applicant is unable to sign this form, he/she may have someone sign and certify on applicant's behalf.
Signing for applicant:______________________________________ Date:_____________________
Print Name:_______________________________Relationship to applicant:___________________________
“DO NOT MAIL IN YOUR COMPLETED APPLICATION”
Page 1 of 1
SPECIAL TRANSPORTATION SERVICE (STS) APPLICATION FORM
III.MEDICAL VERIFICATION (to be completed by a Florida licensed physician)
The Americans with Disabilities Act of 1990 (ADA) requires all public entities operating
STS Eligibility Criteria:
Applicants shall be individually evaluated, and eligibility shall be determined based on a functional ability to use conventional public transportation: Metrobus, Metrorail, and Metromover. Functional inability to use public transportation includes the Americans with Disabilities Act (ADA) Categories 1, 2, and 3 as described in this application.
A. AMERICANS WITH DISABILITIES ACT (ADA) CATEGORIES:
Check the categories of eligibility that you recommend should apply.
1.[ ] The individual is unable, as a result of a physical or mental impairment (including a vision impairment), and without the assistance of another individual, (except the operator of a wheelchair lift or other boarding device), to board, ride, or disembark from an accessible bus or rail vehicle.
2.[ ] The individual needs the assistance of a wheelchair lift or other boarding assistance device and is able, with such assistance, to board, ride, and disembark from accessible transit vehicles. (The individual would be eligible if an accessible vehicle is not available.)
3.[ ] The individual has a specific
4.[ ] Check here, if none of these categories apply.
Medical Representative’s Letterhead Or Prescription Form Requirement:
In order to process this applicant’s request to become a qualified STS rider, we require that the medical certification section of this form be completed, and a letterhead or prescription form with the name and address of both the medical representative and the applicant be attached to this application. To expedite applicant processing, please attach objective medical findings which substantiate the disability. Examples include:
EEG or Neuropsychological Evaluation with FSIQ
Snellen (visual accuity) and/or Perimeter Chart (field of vision) Report(s)
Elisa Western Blot result reading CD4 + counts
Respiratory FVC/FEV1
“DO NOT MAIL IN YOUR COMPLETED APPLICATION”
Page 2 of 2
SPECIAL TRANSPORTATION SERVICE (STS) APPLICATION FORM
III.MEDICAL VERIFICATION (To be completed by a licensed physician)
B.INDICATE THE TYPE AND NATURE OF THE INDIVIDUAL’S DISABILITY(IES).
CHECK AS MANY ITEMS AS MAY BE APPLICABLE. (SEE STS ELIGIBILITY CRITERIA)
1.MOBILITY IMPAIRMENT:
a.[ ]
b.[ ] Ambulatory disability(ambulation may be limited, but able to walk with or without mobility aid, may use wheelchair but can transfer to a seat with little or no assistance).
I. Amputation (detail extremity): _______________________________________________________
II. [ ] Stroke without Hemiplegia III. [ ] Stroke with Hemiplegia IV. [ ] Brain/Spinal Nerve Trauma V. [ ] Other: _________________________________________
Date disability started: _______________ (Please attach EEG or neuropsychological evaluation report)
2. NEUROLOGICAL DISABILITY(motor dysfunction):
(Please attach EEG or neuropsychological evaluation report) |
|
|||
a. [ |
] Multiple Sclerosis |
b.[ ] Epilepsy |
c. [ ] Muscular Dystrophy |
d. [ ] Cerebral Palsy |
e. [ |
] Parkinson’s |
f. [ ] Alzheimer’s |
g. [ ] Other _____________________________________ |
|
3.VISUAL DISABILITY:
a.[ ] Totally blind
b.[ ] Legally blind, If this person is legally blind complete the following:
Corrected visual acuity: |
Right Eye_____ Left Eye_____(Please attach Snellen reports both eyes) |
Corrected field of vision: |
Right Eye_____ Left Eye_____(Please attach Perimeter chart reports both eyes) |
4.COGNITIVE DISABILITY: a.Type of mental impairment:
[ |
] Emotional |
[ |
] Autism |
[ |
] Adult retardation |
[ ] Dementia |
|
|
[ |
] OBS |
[ |
] Alzheimer’s |
[ |
] Developmental disability |
[ |
] |
Other |
___________________
(Please attach EEG or neuropsychological evaluation showing full scale intelligent quotient “FSIQ” or mental age,
as applicable.) |
|
|
|
|
b. Level of mental impairment: |
[ |
] Mild |
[ |
] Moderate [ ] Severe [ ] Profound, I.Q.:________ |
5. UNCONTROLLED FATIGUE: |
|
|
(Must Specify) |
|
a.[ ] Radiation/Chemo b.[ ] Dialysis |
If either |
a. or b. is marked please provide the following: |
||
Treatment Schedule (or duration): ________ |
Treatment Start & expected End date: ______ thru ______ |
|||
Treatment Center: ________________________________ Address: _________________________________
c.[ ] HIV (Please attach Elisa, Western Blot result reading CD4+ counts.) d.[ ] Other _________________
6.IMPAIRMENT RELATED CONDITION:
a. [ ] Arthritis (Please attach
{Functional Classification ____ Anatomical Stage ____} |
b. [ ] Other________________ |
b. [ ] Cardiac (Please attach EKG or operative findings) |
_________________________ |
{Functional Classification ____ Therapeutic Classification ____} |
_________________________ |
c.[ ] Respiratory (Must specify) {FVC ____ FEV1 ____} (Please attach oxymetric capability report)
C. DESCRIBE IN DETAIL THE APPLICANT’S PRIMARY DISABILITY: (BE SPECIFIC)
_____________________________________________________________________________________________
_____________________________________________________________________________________________
______________________________________________________________________________________________________
D. IS THIS DISABILITY: [ ] Perm [ ] Temp; (If temporary, date of disability ________, & length of recovery _______)
E. IS THIS DISABILITY CONTROLLED BY MEDICATION? [ ] Yes [ ] No
Explain:____________________________________________________________________________________
“DO NOT MAIL IN YOUR COMPLETED APPLICATION”
Page 3 of 3
SPECIAL TRANSPORTATION SERVICE (STS) APPLICATION FORM
III.MEDICAL VERIFICATION (To be completed by a licensed physician)
F. INDICATE THE TASKS RELATED TO USING PUBLIC TRANSIT THAT THE APPLICANT WOULD FIND IMPOSSIBLE (NOT DIFFICULT) TO DO. CHECK ALL THAT APPLY:
[ |
] No limitations that would prevent the use of bus/rail service |
[ |
] Enduring warm weather |
[ |
] Boarding vehicle without a wheelchair lift |
[ |
] Waiting thirty minutes |
[ |
] Enduring common weather conditions |
[ |
] Recognizing a bus stop |
[ |
] Identifying a public transit vehicle |
[ |
] Recognizing destinations if stops are |
[ |
] Understanding/handling bus fare (money) transactions |
|
announced |
[ |
] Handling changes in normal routine |
[ |
] Climbing |
[] Walking more than ______ blocks (Must stipulate number of blocks)
These limitations apply: |
[ ] Always |
[ |
] Usually |
[ ] Occasionally [ |
] Rarely |
|
|
G. MOBILITY AID: [ |
]Wheelchair |
[ |
]Walker |
[ |
]Crutches |
[ ]Braces |
[ ]Service Animal |
[ ]None |
[ ] Cane |
[ |
]Other _____________________ |
||||
H. REQUIRED MODE OF TRANSPORTATION: Please indicate the type of transportation required by the applicant based on his/her functional ability.
[ ] Ambulatory (van, sedan) [ ] Wheelchair Transferable(van,sedan) [ ] Wheelchair Confined(lift van)
I. BASED ON THE INDIVIDUAL'S DISABILITY, DO YOU RECOMMEND HIM/HER TO BRING A
PERSONAL CARE ATTENDANT ON EACH TRIP? |
[ ] Yes [ ] No |
J. PLEASE ATTACH PERTINENT MEDICAL DOCUMENTATION (E.G. EVALUATIONS, TEST RESULTS, NOTES, REPORTS, ETC.) THAT WOULD HELP TO EXPLAIN THE DIAGNOSIS OR LIMITATIONS ON THE APPLICANT'S ABILITY TO USE METROBUS, METRORAIL, OR METROMOVER.
NOTE: Failure to attach documentation will delay the eligibility determination process and will require that MDT contact your office to obtain pertinent documentation before rendering a decision.
IN SIGNING, I ACKNOWLEDGE THAT, TO THE BEST OF MY KNOWLEDGE, THE INFORMATION IN THIS EVALUATION FORM IS TRUE AND CORRECT. FURTHERMORE, I CERTIFY THAT, I HAVE ATTACHED OBJECTIVE MEDICAL TESTS/DOCUMENTATION WHICH SUBSTANTIATE THE ABOVE STATEMENTS. I UNDERSTAND THAT PROVIDING FALSE OR MISLEADING INFORMATION COULD RESULT IN THE RE- EXAMINATION OF THE ELIGIBILITY STATUS OF THE APPLICANT AS WELL AS PROSECUTION TO THE MAXIMUM EXTENT ALLOWED BY THE LAWS OF THE STATE OF FLORIDA.
[ ] YES, I have attached the required medical documentation
____________________________________________________ |
|
|
Print or Type Name of Physician |
State of Florida License# |
Signature |
________________________________________________________(____)_________(____)__________
Office Address |
City |
State |
Zip Code Telephone |
Fax # |
“DO NOT MAIL IN YOUR COMPLETED APPLICATION”
Page 4 of 4